Downloaded 18 times
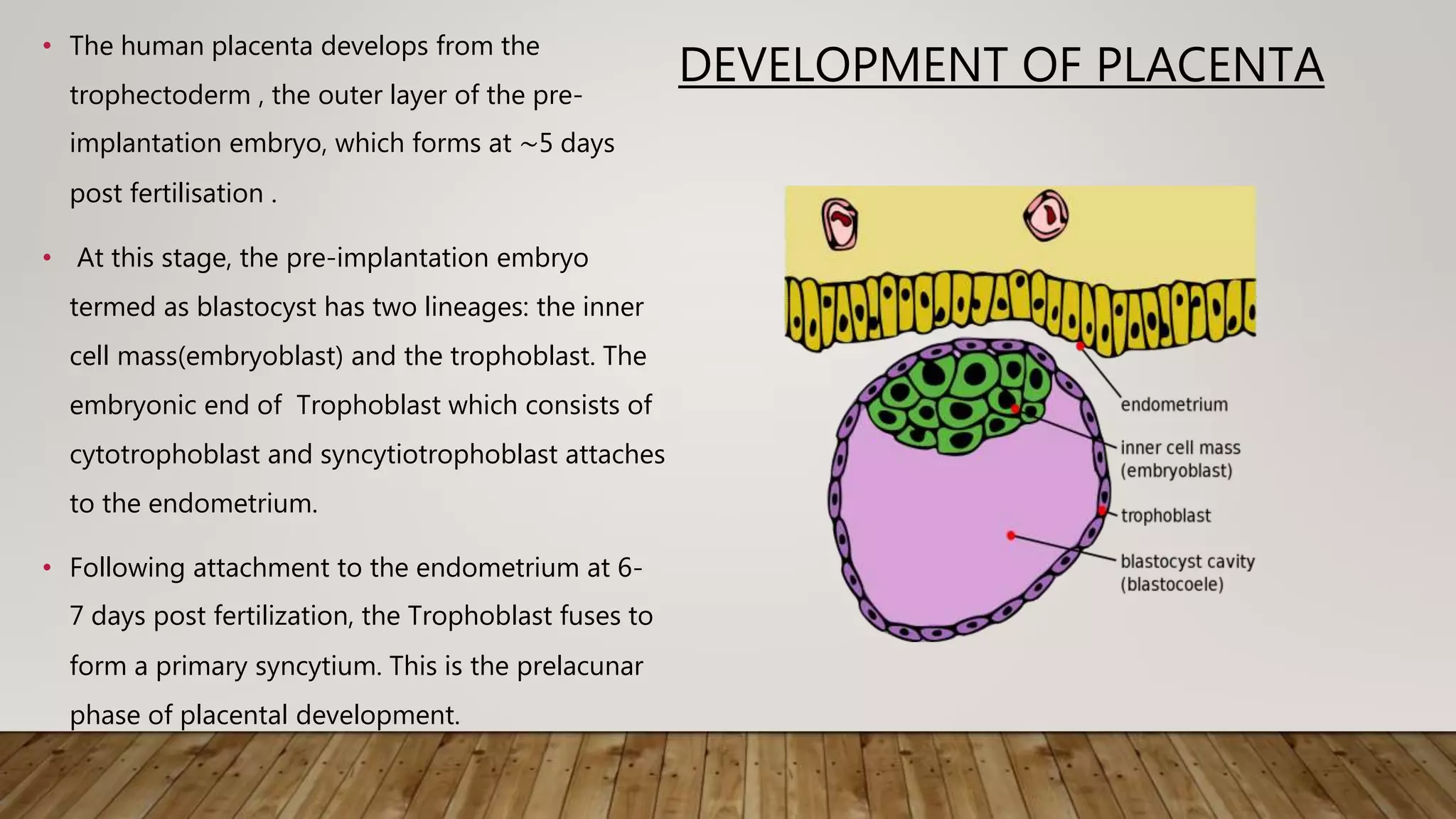
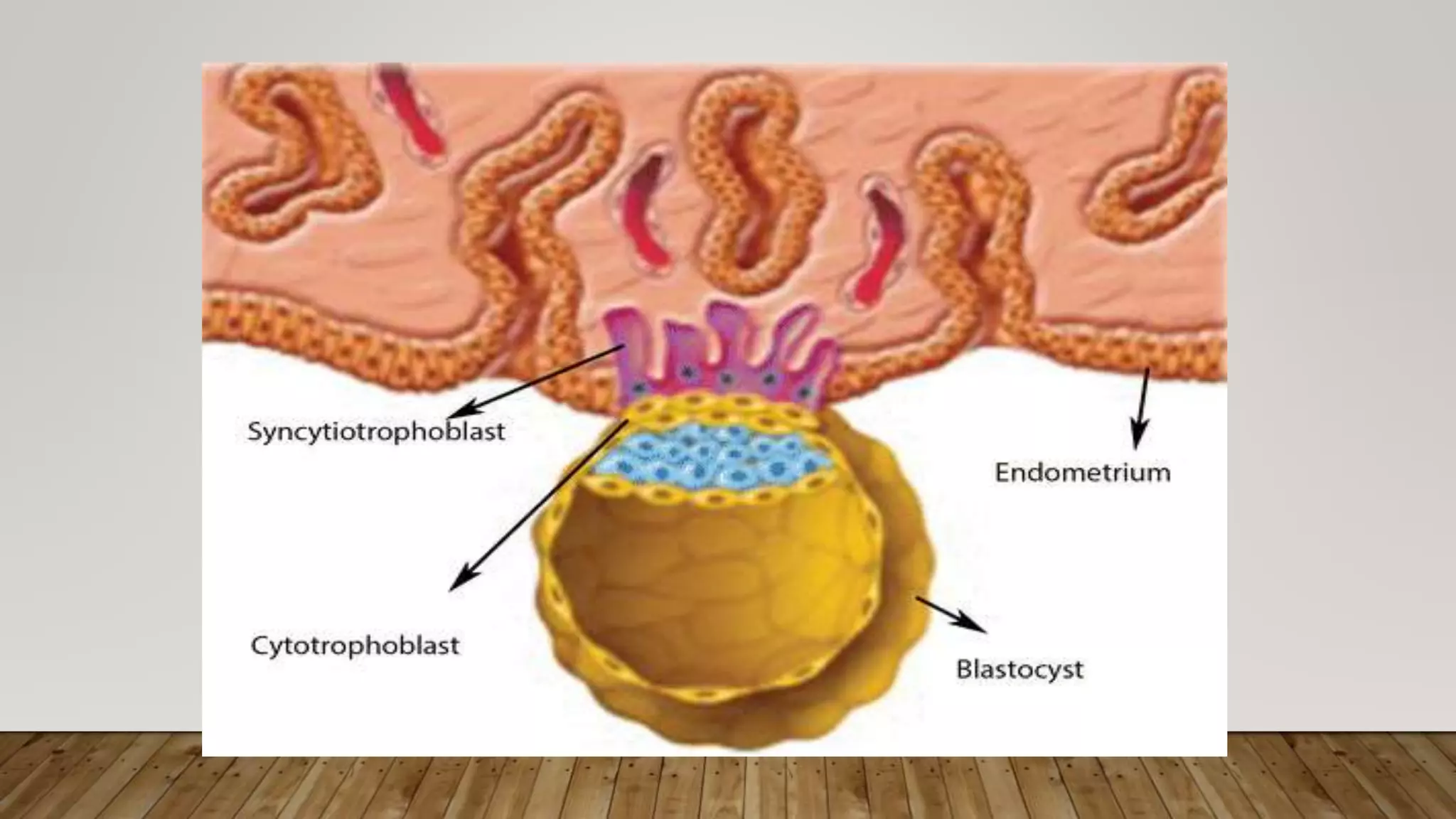
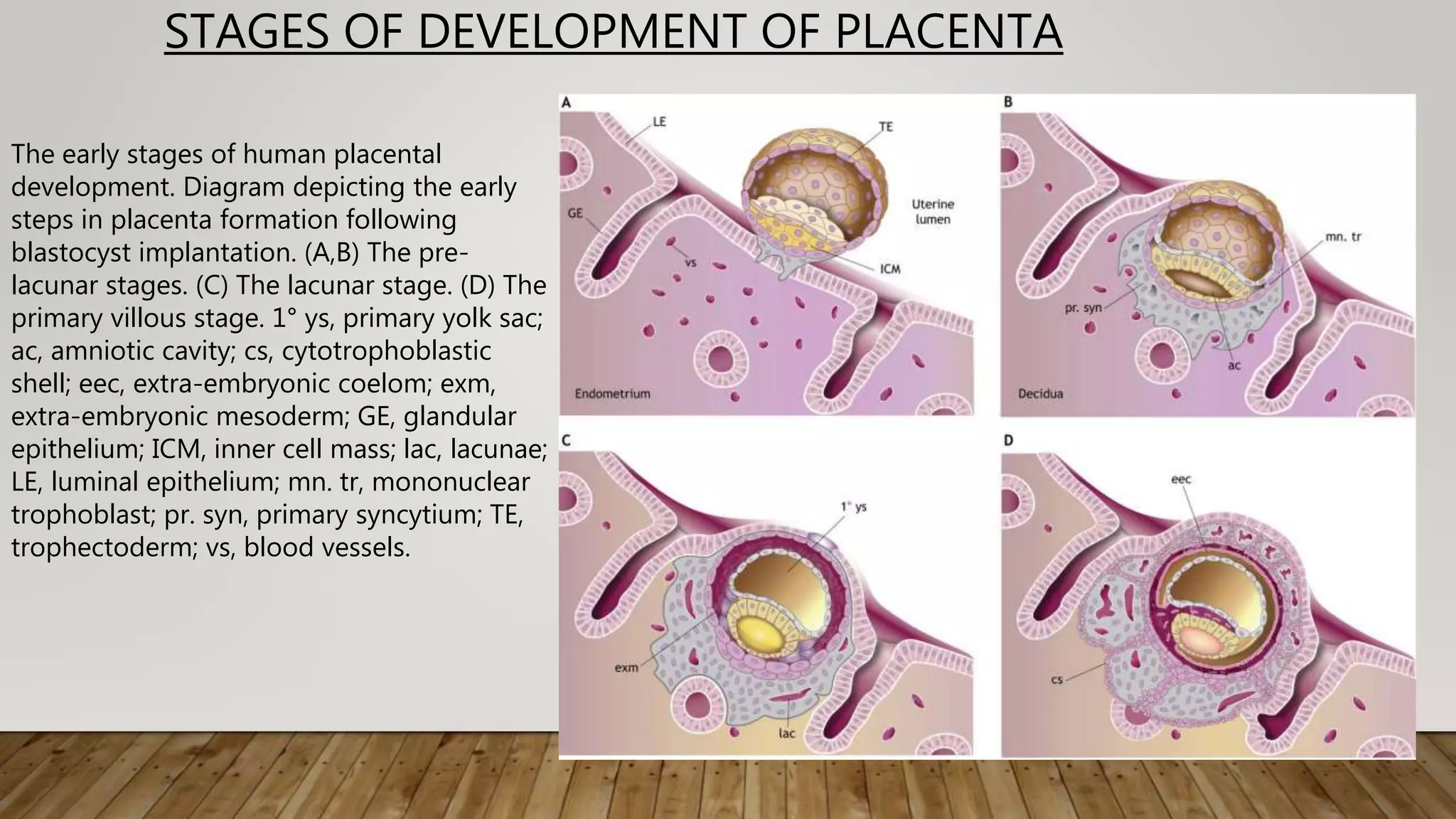

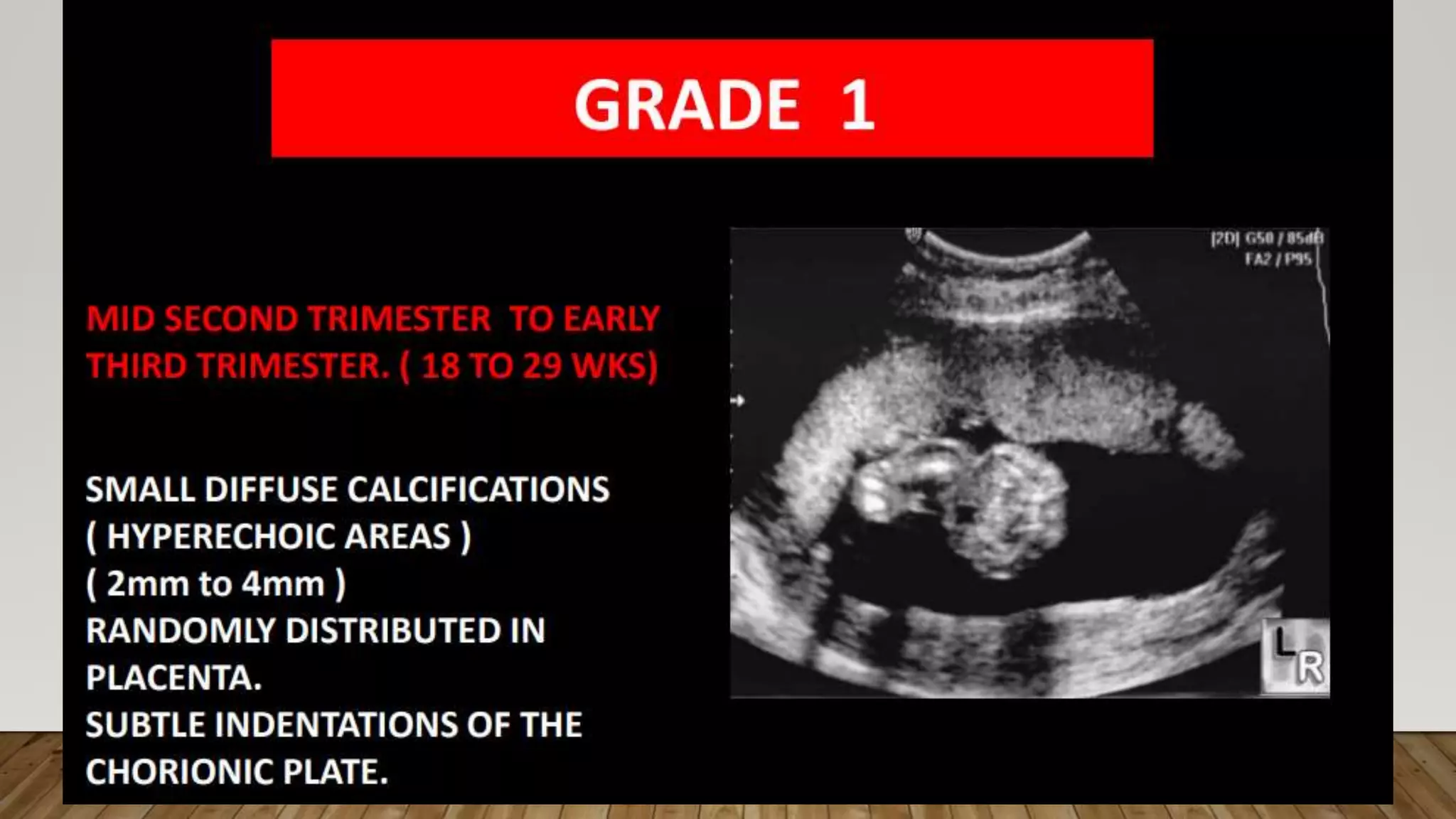
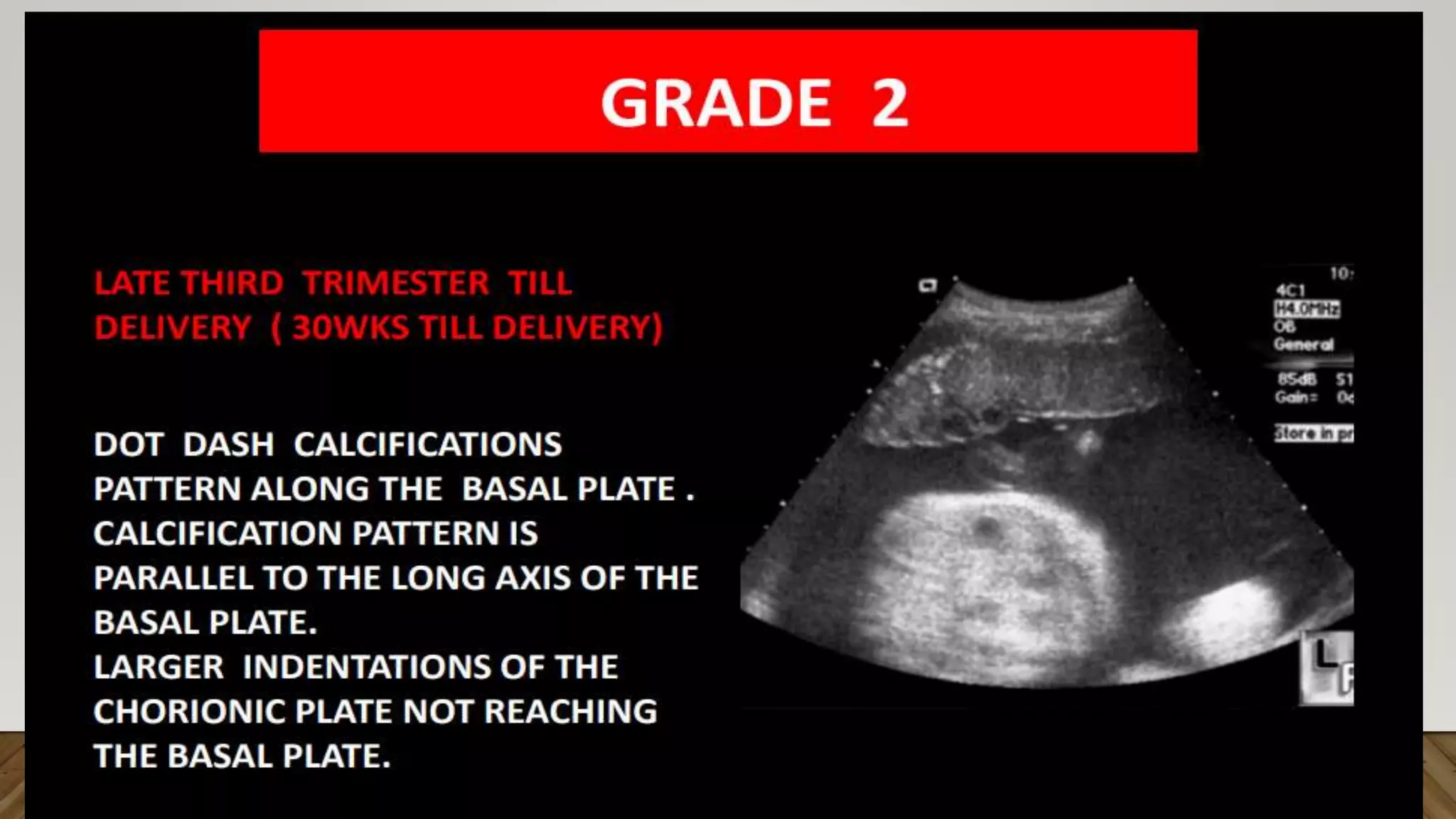
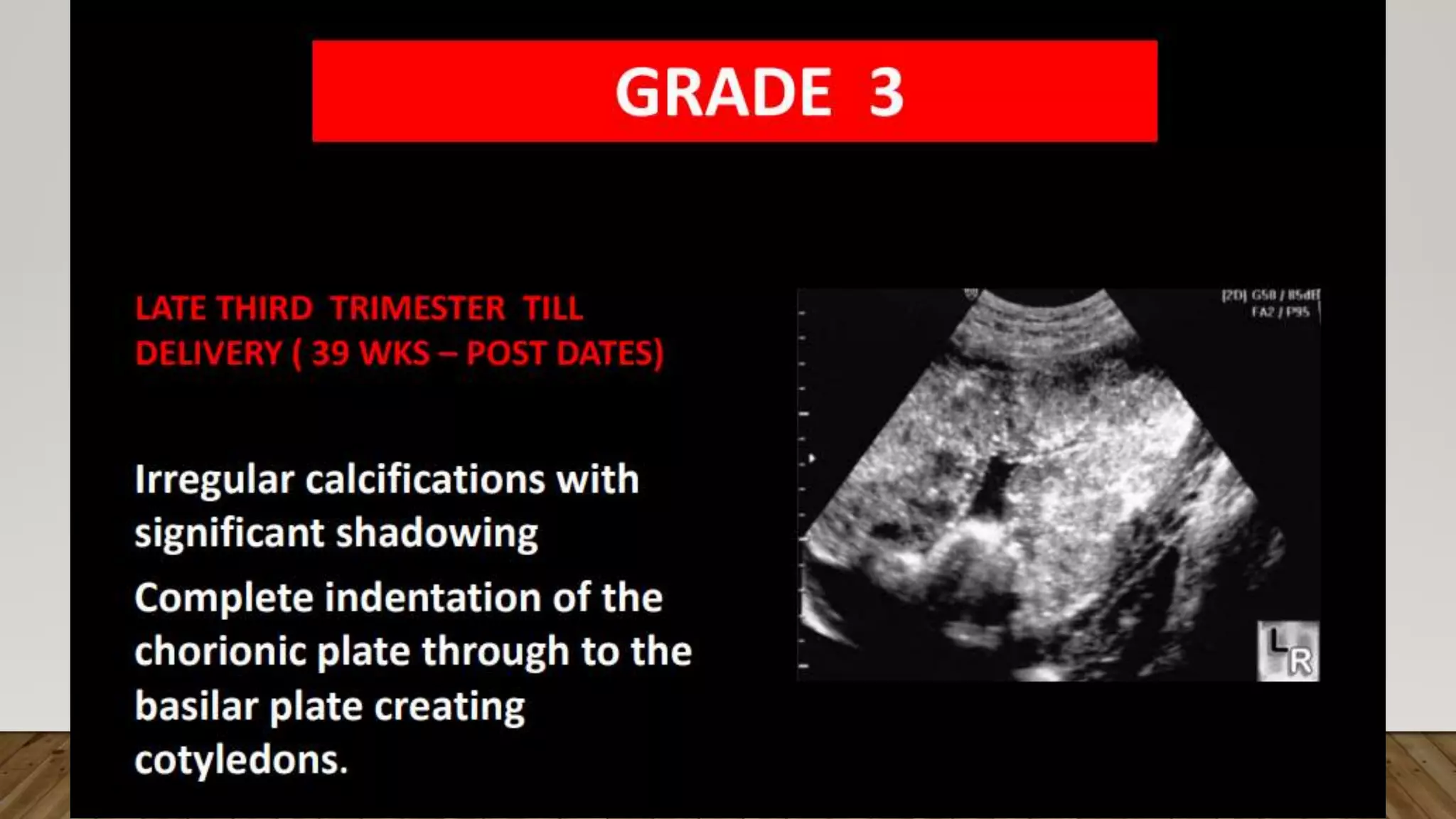
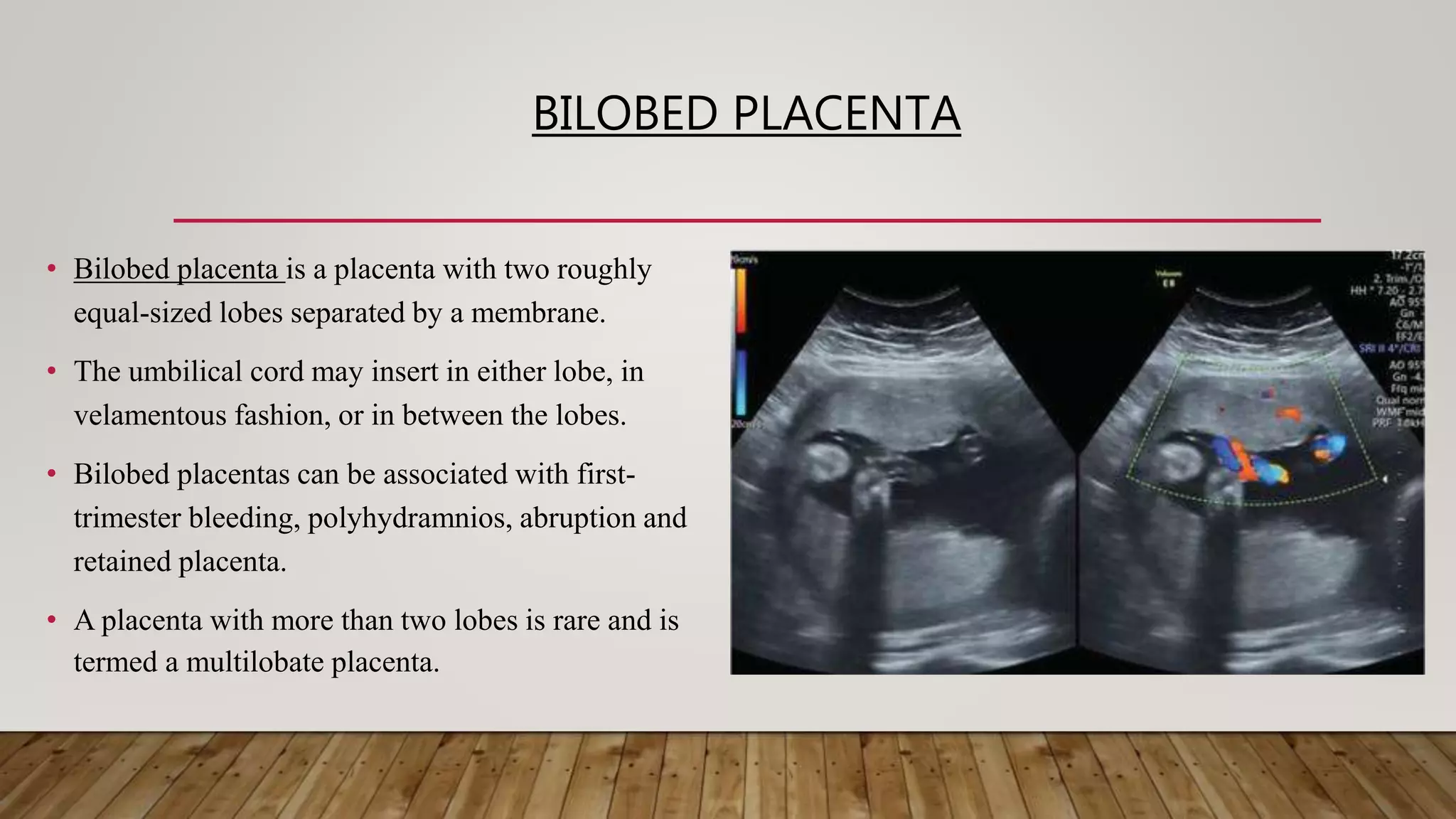


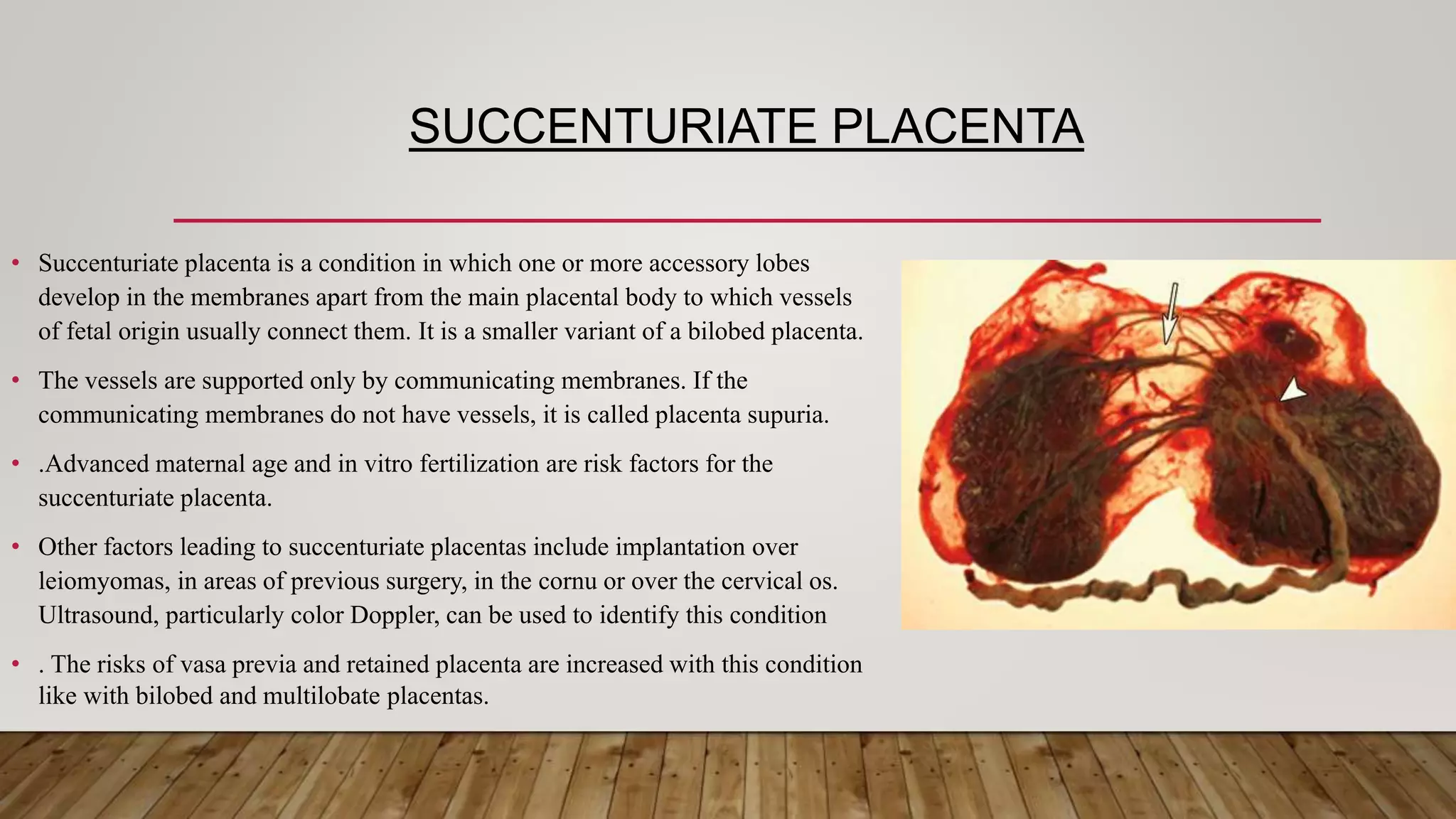

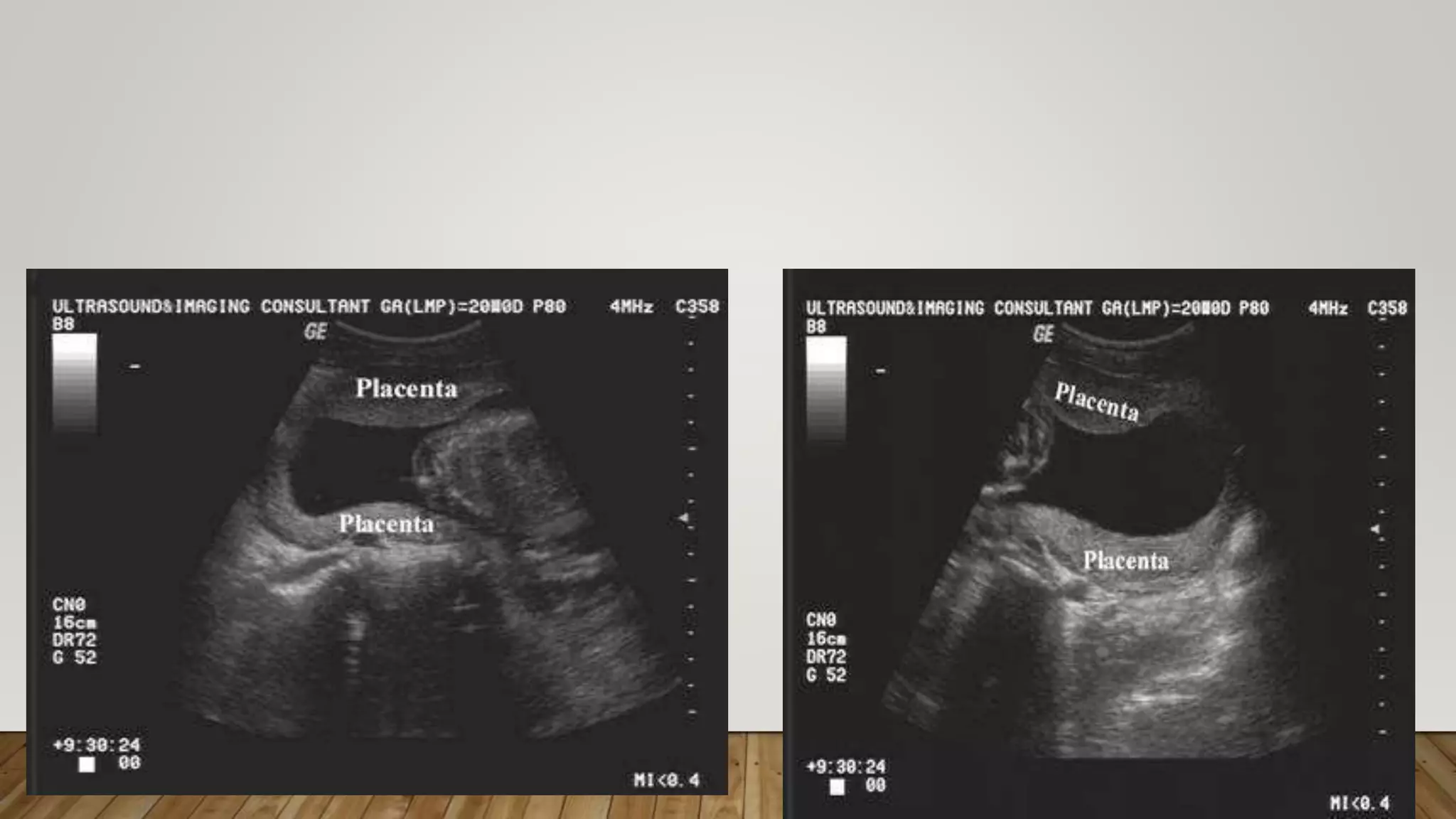



The document discusses the development and types of placentas. It begins by describing the early development of the placenta from the trophoblast cells. It then discusses the stages of placental development including the prelacunar, lacunar, villous, and maturity stages. The document concludes by describing some abnormal placenta shapes including bilobed, circumvallate, succenturiate, membranacea, and ring-shaped placentas. Ultrasound appearance of normal and some abnormal placentas is also presented.