Introduction
• Operative vaginaldelivery refers to a delivery in
which the operator uses forceps or a vacuum
device to assist the mother in transitioning the
fetus to extra uterine life.
• The instrument is applied to the fetal head and
then the operator uses traction to extract the
fetus, typically during a contraction while the
mother is pushing.
3.
• The firstinstrumental deliveries were performed
to extract fetuses from parturient who were at
high risk of maternal mortality due to
prolonged and/or obstructed labor.
• In these cases, saving the mother's life took
precedence over possible harm to the fetus.
• The focus of these procedures has changed
4.
• Decisions regardinguse of instrumental delivery
are now based primarily upon
• the fetal/neonatal impact
• Decisions are also weighed against the
alternative options :-
– cesarean birth,
– prolonging the second stage,
– second stage augmentation
CHOICE OF INSTRUMENT
•The choice of instrument is determined by
level of training with the various forceps
and vacuum equipment.
• Factors that might influence choice are:-
the availability of the instrument,
the degree of maternal anesthesia, and
knowledge of the risks and
benefits associated with each
7.
• In general,vacuum devices are:-
easier to apply,
place less force on the fetal head,
require less maternal anesthesia,
result in less maternal soft tissue trauma,
do not affect the diameter of the fetal
8.
• The advantagesof forceps :-
are unlikely to detach from the head,
can be sized to a premature cranium,
may be used for a rotation,
result in less cephalohematoma
and retinal hemorrhage,
and do not aggravate bleeding from
9.
Summary
• Vacuum deliveryis probably safer than
forceps for the mother, while forceps are
probably safer than vacuum for the fetus.
10.
Forceps Delivery
• Trueforceps were first devised in the late
16th or beginning of the 17th century.
• Hundreds of different forceps available
• Special Vs Classic
11.
Design of Forceps
•basically consist of two crossing
branches.
• Each branch has four
components:
1. blade,
2. shank,
3. lock,
4. handle.
12.
Each bladehas two curves :-
• The cephalic curve conforms to the shape of
the fetal head, and
• The pelvic curve corresponds more or less to
the axis of the birth canal
• Some varieties are
– fenestrated or
– pseudofenestrated to permit a firmer hold on
the fetal head.
13.
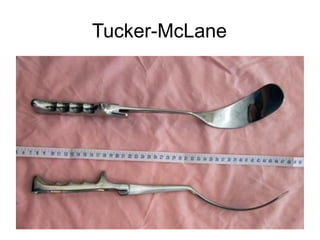
The blades areconnected to the
handles by the shanks, which are either
– Parallel as in Simpson forceps, or
– Crossing as in Tucker–McLane forceps.
The common method of articulation,
1.The English lock, consists of a socket
located on the shank at the junction with
the handle, into which fits a socket
similarly located on the opposite shank
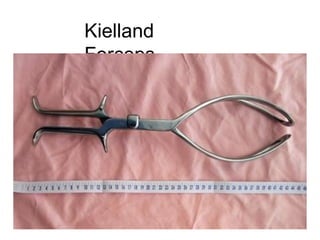
2.A sliding lock is used in some forceps,
such as Kielland forceps
CLASSIFICATION OF FORCEPS
DELIVERIES
•ACOG redefined the classification of forceps
delivery in 1988 to better reflect the degree of
difficulty and attendant risk
• eg, lower fetal station and smaller degrees of
head rotation are associated with reduced
maternal and fetal injury
• classification emphasizes two most important
factors:
Station (O to +5) and
rotation (< / > 45 degree )
18.
CLASSIFICATION OF FORCEPS
DELIVERIES
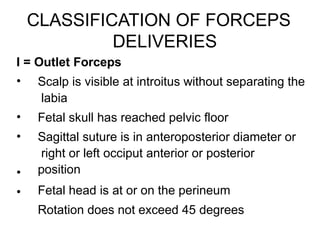
I= Outlet Forceps
•
•
•
•
•
Scalp is visible at introitus without separating the
labia
Fetal skull has reached pelvic floor
Sagittal suture is in anteroposterior diameter or
right or left occiput anterior or posterior
position
Fetal head is at or on the perineum
Rotation does not exceed 45 degrees
19.
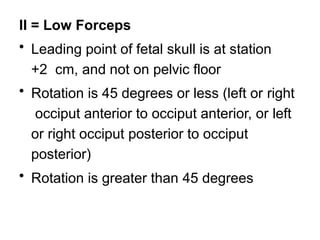
II = LowForceps
• Leading point of fetal skull is at station
+2 cm, and not on pelvic floor
• Rotation is 45 degrees or less (left or right
occiput anterior to occiput anterior, or left
or right occiput posterior to occiput
posterior)
• Rotation is greater than 45 degrees
20.
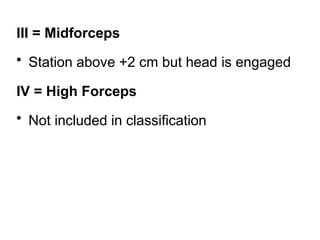
III = Midforceps
•Station above +2 cm but head is engaged
IV = High Forceps
• Not included in classification
21.
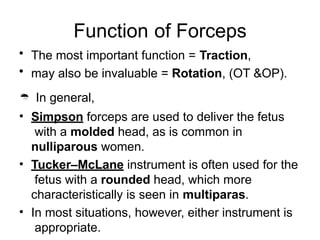
Function of Forceps
•The most important function = Traction,
• may also be invaluable = Rotation, (OT &OP).
In general,
• Simpson forceps are used to deliver the fetus
with a molded head, as is common in
nulliparous women.
• Tucker–McLane instrument is often used for the
fetus with a rounded head, which more
characteristically is seen in multiparas.
• In most situations, however, either instrument is
appropriate.
22.
Indications for forcepsdelivery
• Maternal exhaustion
• Inadequate maternal expulsive efforts
– E.g. - spinal cord injuries or neuromuscular diseases
• Need to avoid maternal expulsive efforts
– E.g. – cardiac or cerebrovascular diseases
• Lack of maternal expulsive effort
• Fetal distress (NRFHRP)
• Prolonged 2nd stage of labor
23.
Contraindications
•
•
•
•
•
•
•
– Are relatedto the potential for unacceptable fetal
risks.
Fetal prematurity
–is a relative contraindication.
Known fetal demineralizing diseases
– (eg, osteogenesis imperfecta),
Fetal bleeding diatheses
– (eg, hemophilia, alloimmune
thrombocytopenia),
Unengaged head,
Unknown fetal position,
Malpresentation
– (eg, brow, face), and
Suspected fetal-pelvic
24.
Pre-requisites for forcepsdelivery
1. Presentation must be vertex or by face
with the chin anterior (L/R MA)
2. Head must engaged.
3. The position of the head must be
known
4. The cervix must be fully dilated.
5. The membranes should be ruptured
6. Adequate pelvis
25.
• Other prerequisitesinclude:
-
-
-
-
Informed consent
Emptying the urinary bladder
Appropriate analgesia
Adequate facilities and back up
personnel
-
Knowledge, experience and skill in
the use of the instrument and manage
complications!!!!!
26.
Forceps application
• Thelong axis of the blades should corresponds
to the occipitomental diameter
• Three forms of application or grip are
recognized
1. Biparieto-malar – Optimal
2. Front-mastoid – Suboptimal
- compresses the mastoid area and the origin of
the facial nerve.
3. Fronto-occipital
– is asymmetric, unsafe and should not be
used.
27.
Steps in Outletforceps delivery
• Precise knowledge of the position of the
fetal head is essential to a proper cephalic
application.
• Insert the left blade first.
28.
1. Two ormore fingers of the right hand are
introduced inside the left, posterior portion of
the vulva and into the vagina beside the
fetal head.
2. The handle of the left branch is grasped
between the thumb and two fingers of the left
hand, and the tip of the blade is gently passed
into the vagina between the fetal head and
the palmar surface of the fingers of the right
hand (serves as a guide).
-The handle and branch are held at first almost
vertically, but they are depressed as the blade
adapts to the fetal head, eventually to a
horizontal position.
29.
3.Similarly, two ormore fingers of the left
hand are then introduced into the right,
posterior portion of the vagina to serve as
a guide for the right blade, which is held in
the right hand and introduced into the
vagina.
4.Then the horizontally positioned branches
are articulated.
5.If necessary, one and the other blade
should be gently maneuvered until the
handles are repositioned to effect easy
articulation.
30.
Traction
•
•
•
•
• The pelvisis curved in a J-shape, and it is in this
direction that the series of force vectors should be
applied.
Traction is always applied gently and never with
excessive force.
More horizontal traction is applied, and the handles are
gradually elevated, eventually pointing almost directly
upwards as the parietal bones emerge.
As the vulva is distended by the occiput, episiotomy
may be done if indicated.
It is preferable to apply traction with each uterine
contraction, except when delivery is urgently indicated.
• Documentation ofProcedure
- Indication, date and time
- The prerequisites
- The estimated fetal weight and the maternal pelvis
- Statement about the FHR and maternal contractions
- Maternal condition and type of anesthesia
- Record of discussion with the woman of the risks, benefits
and options.
- Number of application of forceps, ease of application and
any complication with the application
- Duration and force of each traction attempt and the
number of traction attempts
- Description of maternal or neonatal injuries
- Cord blood gases and Apgar scores
33.
VACUUM DELIVERY
• Isan operative vaginal procedure to facilitate
vaginal delivery with an application of a cup over
the fetal head for brief duration and minimal
traction forces.
• In the United States, the device is referred to as
the vacuum extractor,
• In Europe it is commonly referred to as a
ventouse (from French, literally, soft cup).
34.
Principle
• traction ona metal cap designed = so that
the suction creates an artificial caput, or
chignon, within the cup that holds firmly
and allows adequate traction.
• use a metal or a soft cup (Silastic cap)
Malmstrom = Metal
Mitavac = Soft
CMI tender touch = Soft
Difference?
35.
• Indications andpre-requisites
• -Are generally like that for forceps delivery
– except for :-
face and
after –coming head
36.
• Contra indications
1.Cephalopelvic disproportion
2. High station (above 0-station)
3. Non- vertex presentations
4. Extreme prematurity
5. Known macrosomia
6. Recent scalp blood sampling
37.
Application of VacuumCups
• Proper cup placement is the most
important determinant of success in
vacuum extraction
38.
Ideal application “FlexingMedian” is when :-
•
•
•
•
the center of the cup is superimposed on the flexion point
(3 cm infront of the posterior fontanelle on the
sagittal suture)
the cup is symmetrically placed over the sagittal suture.
If the center of the cup = more than 1cm to either side of
the sagittal suture, the application is described as
paramedian, and
when the application distance is less than 3cm, it is
called
deflexing.
39.
• Thus, thereare four types of cup applications:-
1.Flexing median ( correct/ideal application)
2.Flexing paramedian
3.Deflexing median
4.Deflexing paramedian
• -Deflexing and paramedian applications
promote:-
extension and
asynclitism of the head and
effectively increase or fail to decrease the size
and the area of the presenting part.
40.
Technique for Applicationof Vacuum cup.
•
•
•
•
•
•
First, test the instrument
Recheck the position of the occiput and locate the
flexion point.
Connect cup tubing to the tube of the vacuum pump.
Smear the outside of the cup lightly with obstetric cream.
Press the cup against the fetal head and maneuver until
its center lies over the flexion point
Check that there is no maternal tissue / fetal
electrode
trapped.
41.
Cont…
• Induce avacuum pressure of 20 kpa (0.2
kg/cm2) and recheck the cup position.
• Then increase the vacuum in one step to the
recommended pressure of 80 kpa (0.8 kg/cm2)
• Delay traction for 2 minutes to allow chignon to
form although gentle traction may be
commenced sooner if necessary.
• 0.2kg/2min = rigid cap
• 0.8kg/1min = soft cap
42.
Traction
• Should bedirected in such a way that the flexion
point on the head is aligned with the axis of the
pelvis
• Traction should be a 2- handed exercise
1.The right hand holds the traction handle and
pulling in the direction of descent
2.The thumb of the non- pulling hand presses
against the dome of the cup
43.
“3Ds”
1st pull shouldcause flexion of the head and
some descent = Dislodge
2nd pull the head should be on the pelvic
floor
= Descent
3rd pull delivery of the head should be
complete or imminent = Deliver
44.
Cont…
•
•
•
Traction is discontinued
–betweencontractions or
–if an audible hiss is heard signaling loss of vacuum.
After delivery of the head, the vacuum is released, the
cup eased off the scalp and the birth completed in the
normal manner.
Vacuum extraction should be considered a trial, if there
is no evidence of descent, consider C/S = “3Ds”
Recommendations Regarding VacuumDelivery
The classification of vacuum deliveries should be the
same as that utilized for forceps
The same indications and contraindications utilized for
forceps deliveries should be applied
The vacuum should not be applied to an unengaged
vertex, that is, above 0 station.
The individual performing or supervising the procedure
should be an experienced operator.
The operator should be willing to abandon the
procedure if it does not proceed easily or if the cup
pops off more than three times.
Important features
• Needfew instruments
• Leaves the mother with intact uterus
• If she is already infected, low risk of
spread of infection to the peritoneum
• Shorter time in bed
Rate of DVDin Eth
•
•
•
•
•
•
•
Study done in TAH (1997-2002)
7.8 DVDs per 1000 deliveries
Craniotomy (94%) & for CPD(89%)
Average BW -2957gm
preterm(13%), post term(7%), term (54%)
Labor >24hrs in 88%
– Fistulas , infection & genital trauma
Currently almost never practiced in the
developed world
Prerequisites for DVD
•
•
•
•
•
•
•
Deadfetus
exceptions (malformation or tumor incompatible with life,
Cleidotomy & needle aspiration for hydrocephalus)
Fully dilated cervix
No gross pelvic contracture
No risk of uterine rupture
2/5 or less of his head must be above the brim
Back up operative facilities
53.
CRANIOTOMY
• Perforation ofthe skull and emptying the
head of brain tissue so that the head
collapses.
• It is used when the fetus presents with the
head or in a case of retained head in a
breech
54.
CRANIOTOMY INDICATIONS
• Obstructedlabor with a vertex or face
–
• Arrested after coming head –
• Hydrocephalus-
• Interlocked head of twins –
• Contracted pelvis is the most common
indication
55.
CRANIOTOMY
• Scalp isheld with a tissue forceps and
incision is made with a perforator and contents of the
brain are evacuated.
• Sites-
vertex- parietal bone
face- orbit/hard palate
brow- frontal bone
After coming head- foramen magnum
Hydrocephalus- encephalocentesis
56.
Decapitation
• Cutting theneck and separating the head
from the truncus followed by version and extraction
• Indication :-
1. obstructed labor in shoulder presentation when the neck
is easily accessible,
2. locked twins
• Instrument-
– decapitating wire
57.
Evisceration
• Perforation ofthe truncus (chest or abdomen) with
removal of all internal organs so that the
body collapses and a version and extraction can be
done without the risk of rupturing the uterus.
• Indication-
1. Shoulder presentation where it is difficult to reach the
neck
2. Fetal malformation
- (ascites , huge distended bladder , hydronephrosis)
58.
Evisceration Procedure
•
•
•
•
•
Pull onthe prolapsed arm & his axilla
protect the vaginal wall with speculum
make an opening in the chest or abd. wall
Remove the viscera
– (liver, heart, and lungs)
If necessary perforate his diaphragm with
scissors
59.
Cleidotomy
• Cutting ofone or both clavicles to reduce
the width of the shoulder
• Indication :-
• Shoulder dystocia and other
maneuvers for shoulder dystocia have been
unsuccessful





















![operative_vaginal_delivery[1].pptrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrr...](https://cdn.slidesharecdn.com/ss_thumbnails/operativevaginaldelivery1-241116225613-cf843d5e-thumbnail.jpg?width=640&height=640&fit=bounds)































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)



![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)







