DEFINITION
Obstetric forceps isa pair of instruments
specially designed to assist extraction of the
fetal head and thereby accomplishing the
delivery of the fetal head.
4.
VARIETIES
Long curvedobstetric forceps
Short curved forceps (Wrigley forceps)
Kielland’s forceps
BLADES
There are 2blades. Each blades consist of
the following parts
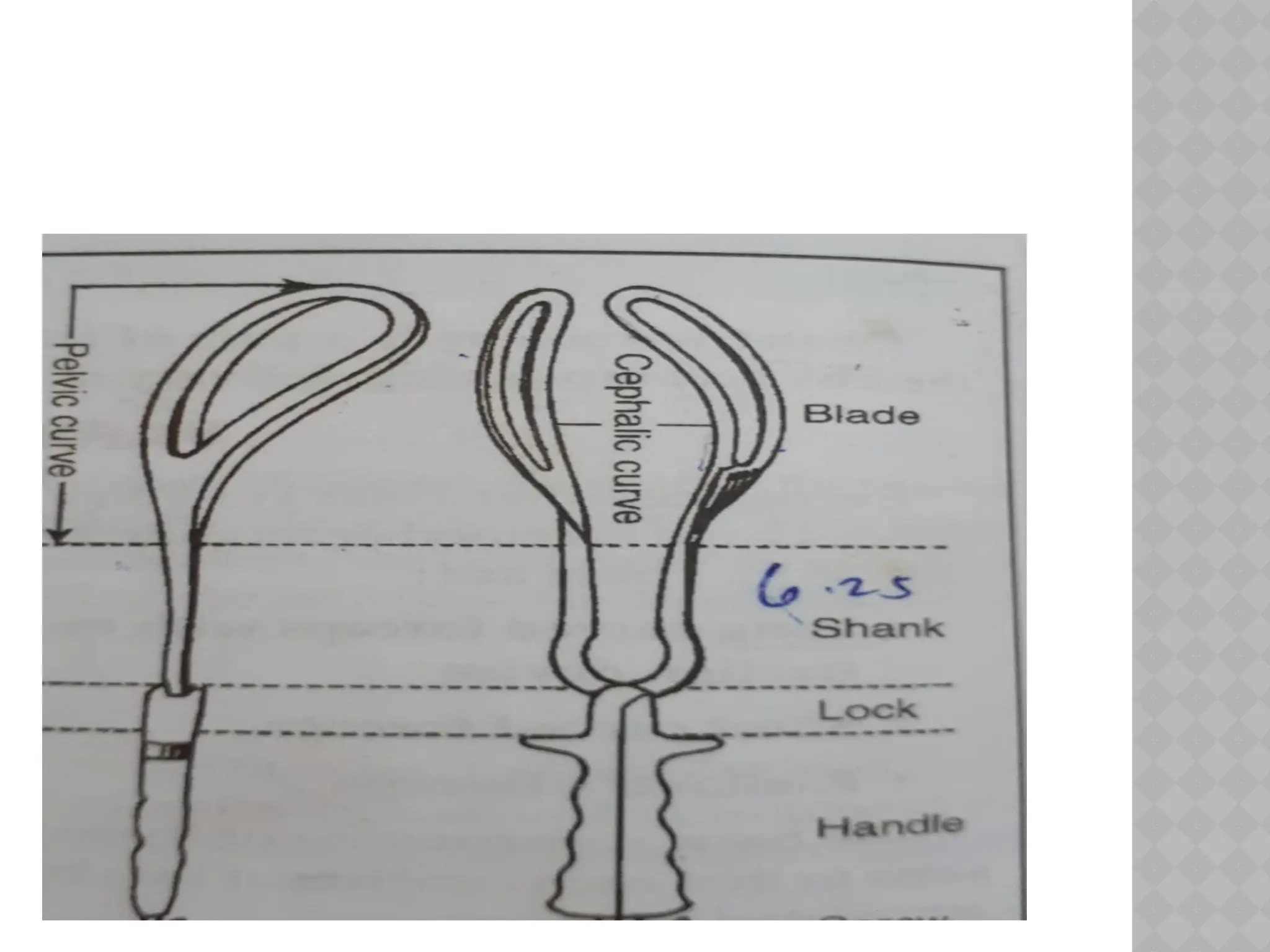
Blade
Shank-6.25 cm.
Lock
Handle with or with out screw-12.5 cm
8.
The blades havegot 2 curves
Pelvic curve:
The curve on the edge is to fit more or less
the curve on the axis of the birth canal
(curve of carus).It forms a part of a circle
whose radius is 17.5 cm.
The front of the forceps is the concave side
of the pelvic curve.
9.
Cephalic curve-
Itis the curve on the flat surface, When
articulated grasps the fetal head without
compression.
The radius of the curve is 11.5 cm.
10.
HOW TO IDETIFYTHE BLADES
When articulated
Place the instrument infront of the pelvis
with the tip of the blade pointing upwards
and the concave side of the pelvic curve
forwards.
The blades corresponds to the left of the
maternal pelvis is the left blade and to the
right side is the right blade.
11.
CONT....
When isolated
Thetip should point upwards
The cephalic curve is to be directed inwards
and the pelvic curve forwards.
12.
CHOICE OF FORCEPSOPERATION
Mid forceps
It is used when the head is at or near the
level of ischial spine.
Low forceps
The head is near the pelvic floor or even
visible at the introitus.
Outlet forceps
Applied when the head is on the perineum
13.
TYPES OF APPLICATIONOF THE
FORCEPS BLADES
Cephalic application: The blades are applied
along the sides of the head grasping the
biparietal diameter in between the widest
part of the blades.
Pelvic application
When the blades of the forceps are applied
on the lateral pelvic walls ignoring the
position of the head is called pelvic
application
14.
FUNCTIONS
The tractionis the important function .The
pull required is to be 18 kg and in multipara
13 kg.
Its compression effect on the cranium is
minimum.
Rotation of the head can be achieved by
keilland’s forceps.
Provide protective cage for the head
15.
INDICATIONS
MATERNAL
Inadequate expulsiveefforts
Maternal exhaustion
Where expulsive efforts are to be
avoided(cardiac disease, eclampsia, cerebral
vascular disease)
FETAL
Non reassuring fetal heart rate
After coming head of breech
16.
OTHERS
Prolonged secondstage of labour
To cut short second stage in severe
preeclampsia,cardiac disease etc..
17.
CONDITIONS TO BEFULLFILLED
FETAL AND UTERO PLACENTAL CRITERIA
Fetal head must be engaged
Cervix must be fully dilated
The membranes must be ruptured
The position and station of the head must be
known.
MATERNAL CRITERIA
No major CPD by clinical pelvimetry
Bladder must be emptied
Adequate analgesia
18.
FORCEPS
F-favourable headposition and station
O-Open Os(fully dilated)
R-Ruptured membranes
C-Contractions present and Consent
E-Engaged head ,Empty bladder
P-Pelvimetry-no major CPD
S-Stirrups, lithotomy position
19.
LOW FORCEPS OPERATION
Preliminaries
Anesthesia- Perineal infiltration with 1% lignocaine
hydrochloride.
Catheterization
Internal examination to assess
-the status of the cervix
-membrane status
-Presentation and position of the head
-Assessment of the pelvic outlet
Episiotomy: done when the perineum becomes
bulged by the head.
20.
STEPS
Identification ofthe blades and their
application
Locking of the blades
Traction
Removal of the blades
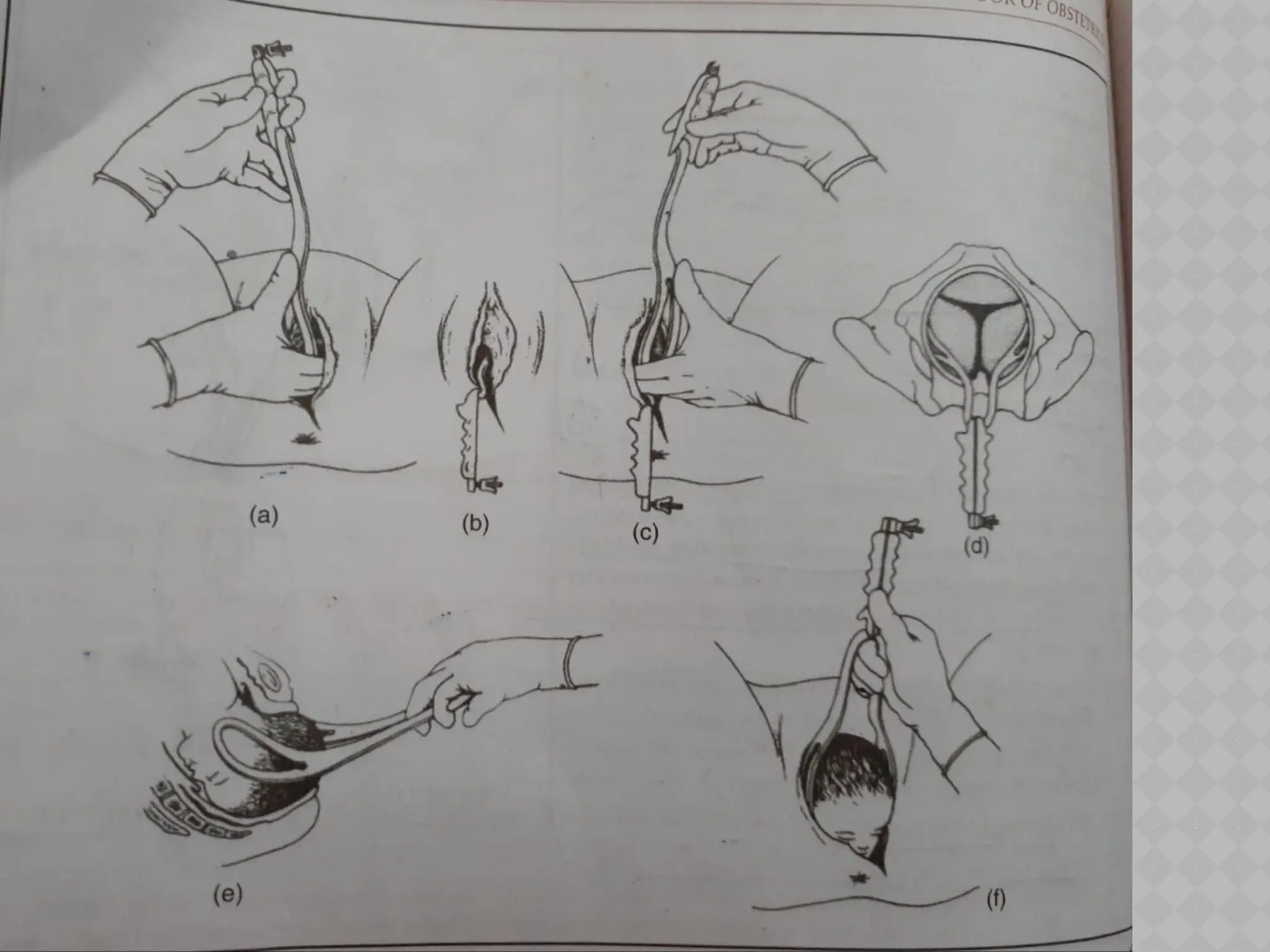
STEP-1:Identification of the blades and their
application
-The blade is identified and the left blade is
introduced first.
-The four fingers of the semisupinated right hand
are inserted along the left lateral vaginal wall.
21.
The palmersurface of the fingers rest
against the side of the head.
The fingers are to guide the blade during
application and to protect the vaginal wall.
The handle of the left blade is taken lightly
by three fingers of the left hand-index,
middle and thump in a pen holding manner
and is held vertically almost parallel to the
right inguinal ligament.
The fenestrated portion of the blade is
placed on the right palm with the tip
pointing upwards.
The right thump is placed at the junction of
the blade and the shank.
23.
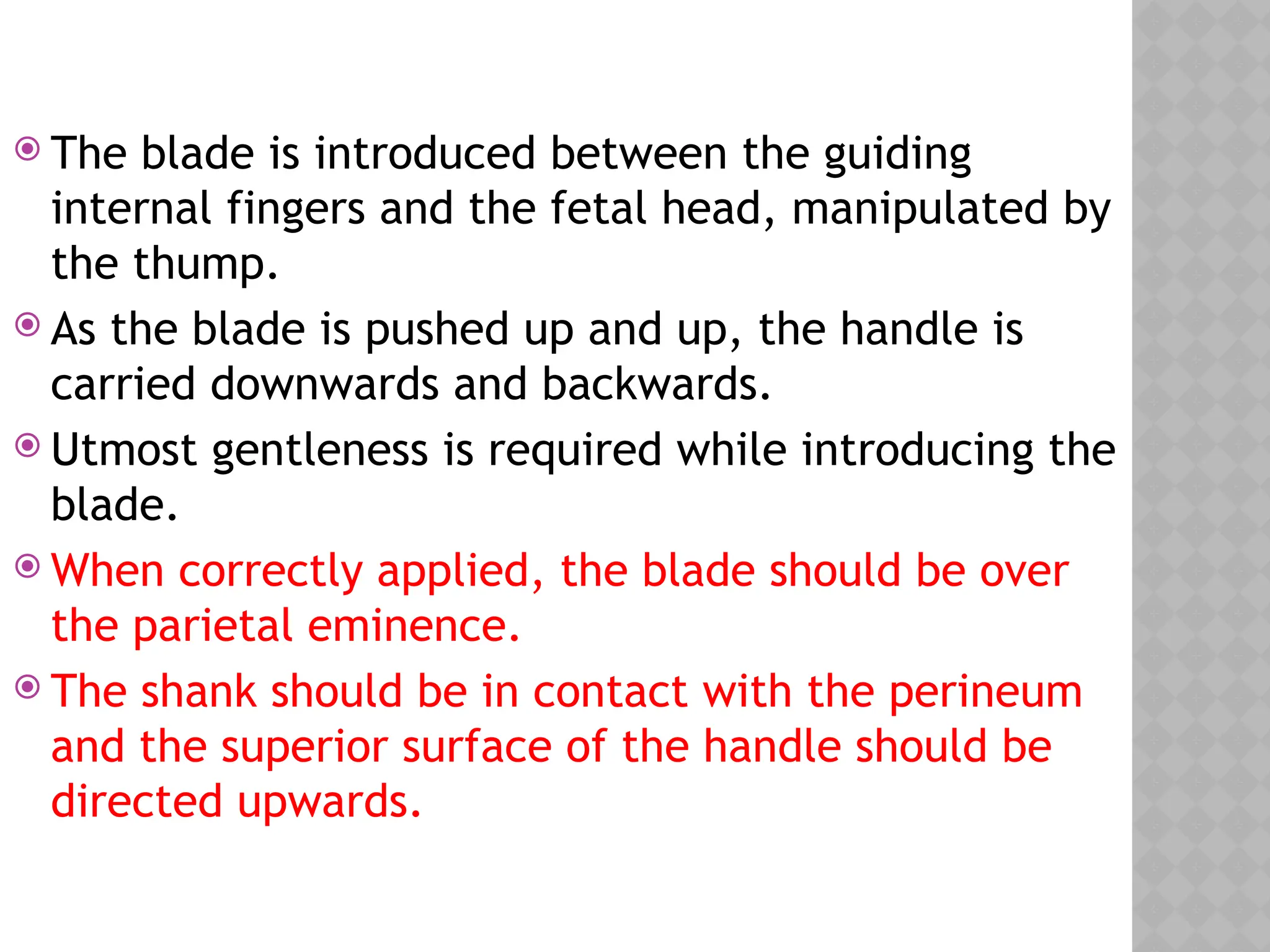
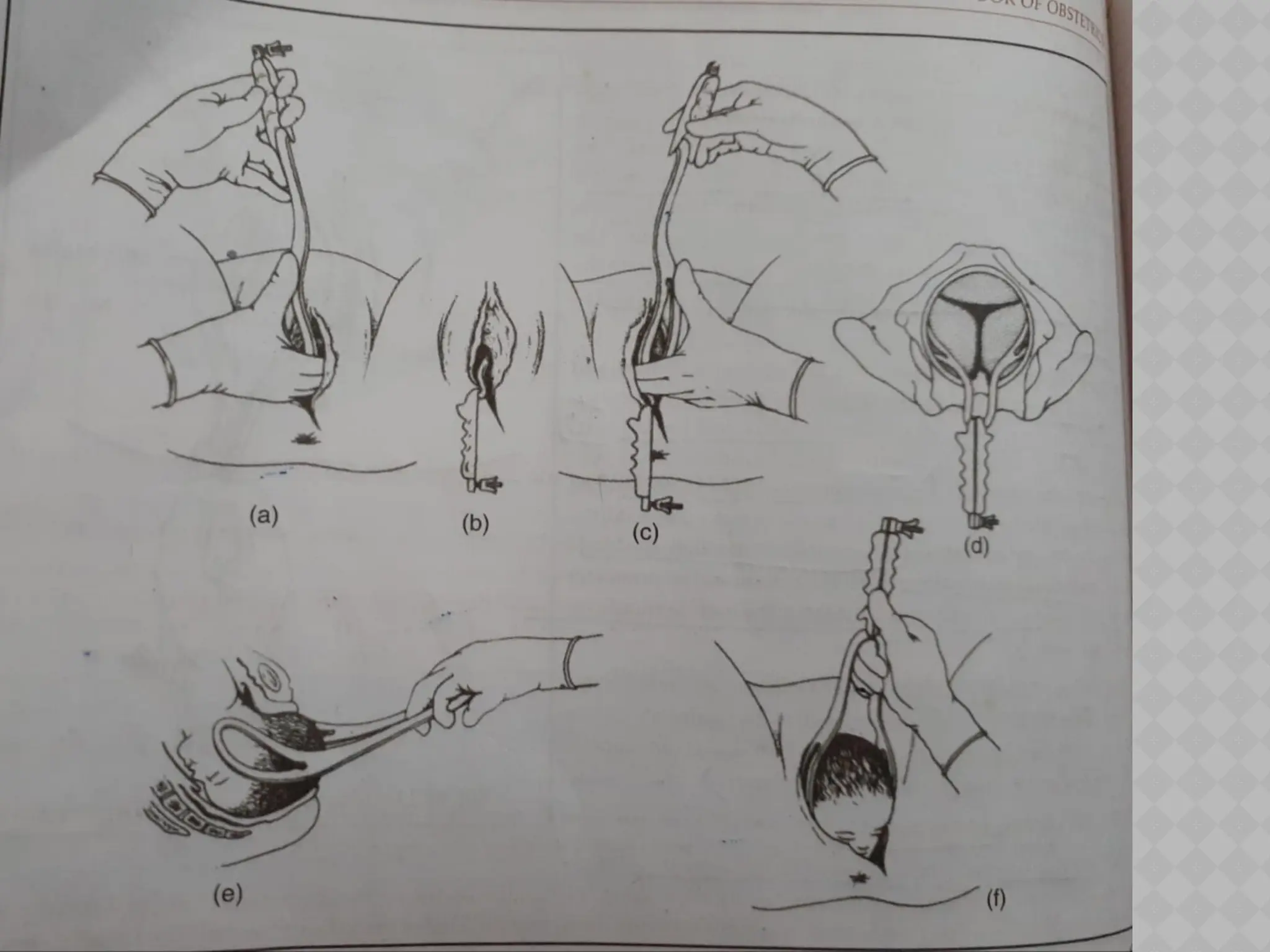
The bladeis introduced between the guiding
internal fingers and the fetal head, manipulated by
the thump.
As the blade is pushed up and up, the handle is
carried downwards and backwards.
Utmost gentleness is required while introducing the
blade.
When correctly applied, the blade should be over
the parietal eminence.
The shank should be in contact with the perineum
and the superior surface of the handle should be
directed upwards.
25.
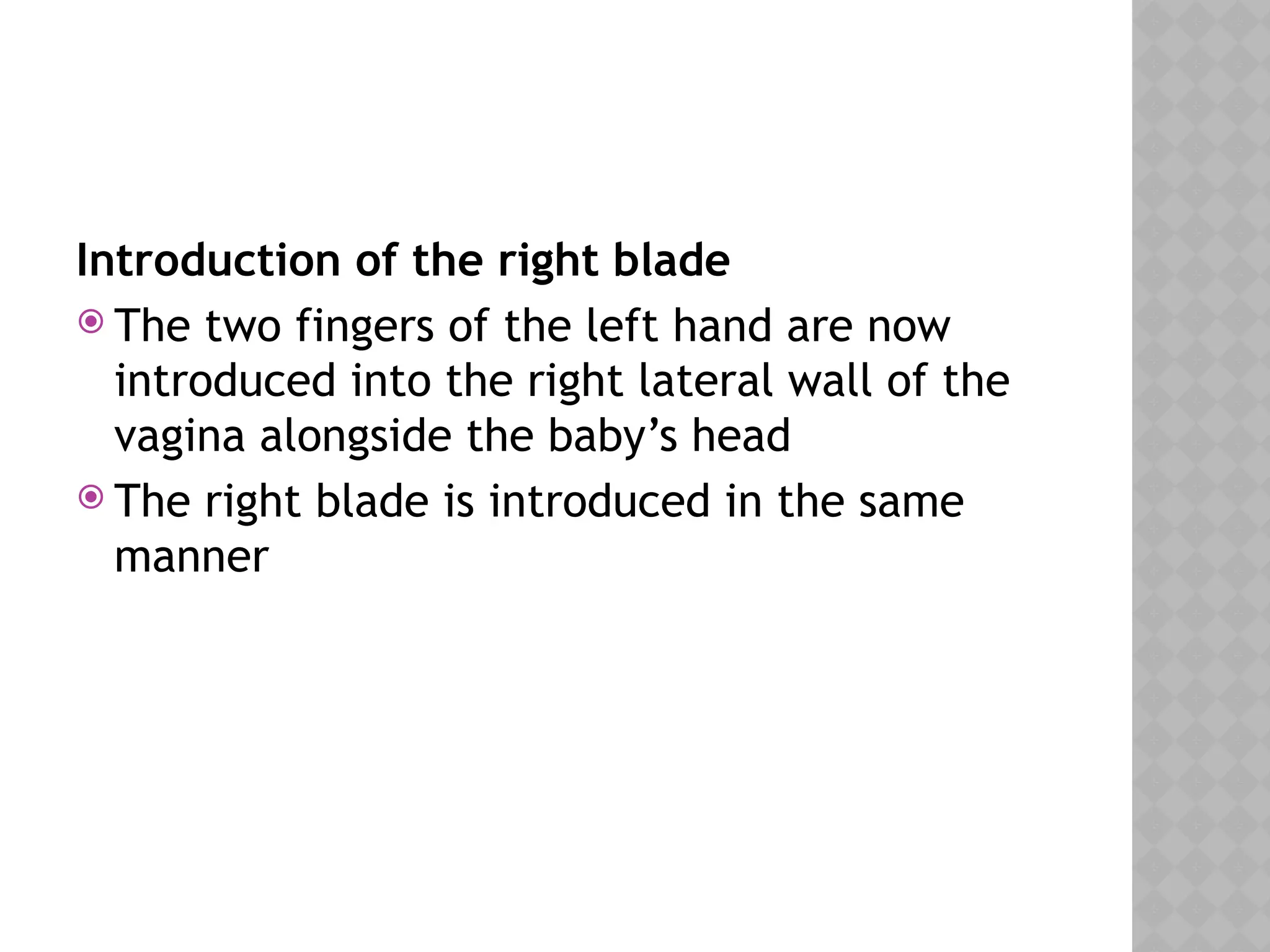
Introduction of theright blade
The two fingers of the left hand are now
introduced into the right lateral wall of the
vagina alongside the baby’s head
The right blade is introduced in the same
manner
26.
STEP –II.LOCKING OFTHE
BLADES
When correctly applied the blades should be
articulated with ease.
27.
STEP-III & IV-TRACTIONAND
REMOVAL OF THE BLADES
Before traction is applied, correct
application is evidenced by
-easy locking
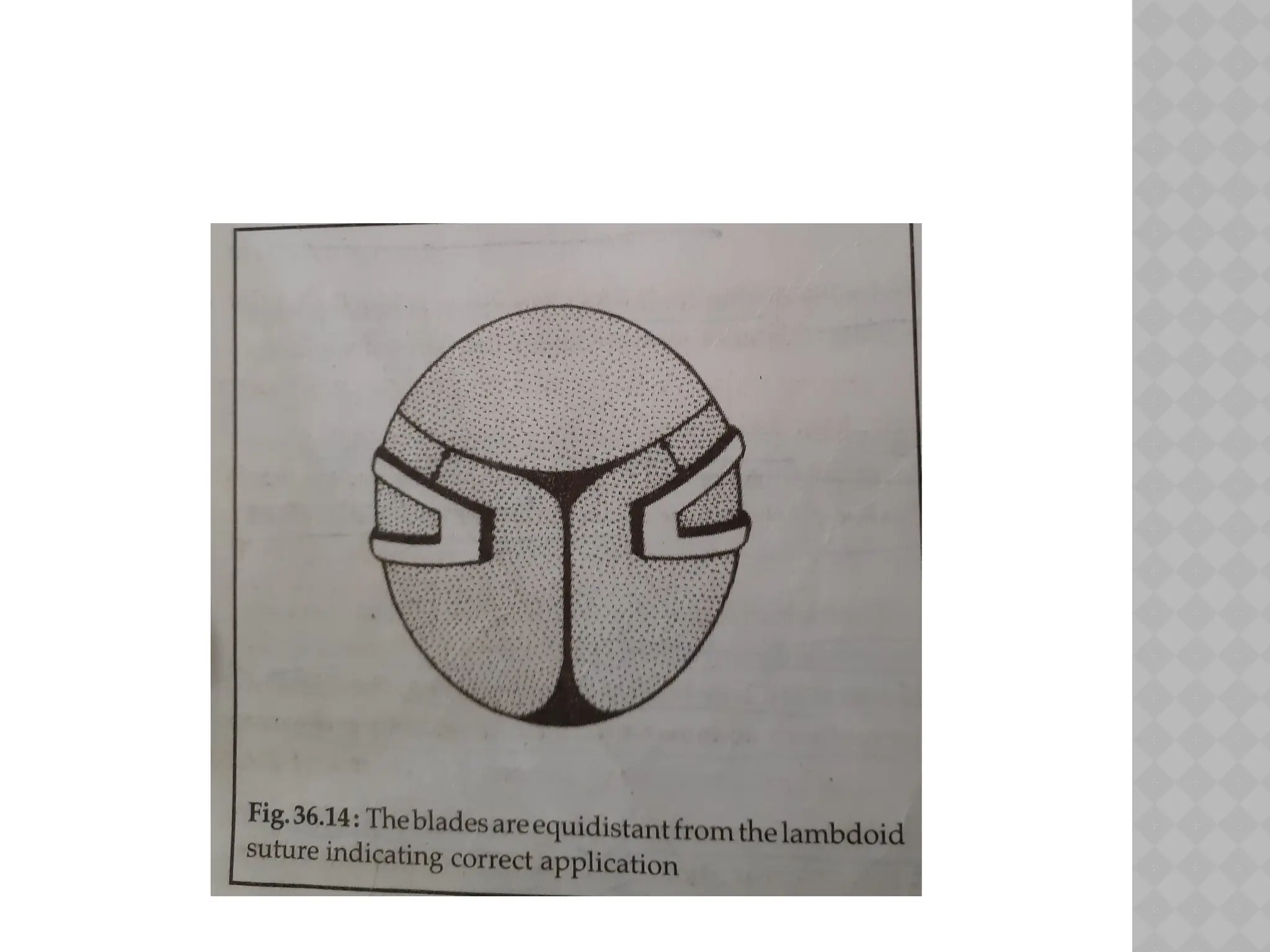
-the blades are equidistant from the lambdoid
suture
-firm grip of the head on the biparietal
diameter.
Principles-Steady but intermittent traction
should be given if possible during
contractions.
29.
Gripping of thearticulated forceps during
traction
The traction is given by gripping the handle,
placing the middle finger in between the
shanks with the ring and index fingers on the
either side of the finger guard.
During the final traction four fingers are
placed in between the shanks and thump
under surface of the handles.
30.
Direction of thepull
The direction of the pull corresponds to the long
axis of the birth canal.
The direction of the pull is downwards and
backwards until the head comes to the perineum.
The pull is then directed horizontally straight
towards operator till the head is almost crowned.
The direction of the pull is gradually changed to
upwards and forwards towards mother’s abdomen
to deliver the head by extension.
The blades are removed one after another.
31.
CONT....
Following thebirth of the head ,usual
procedures are to be taken as in normal
delivery.
Routine intravenous methergin 0.2 mg is to
be administered with the delivery of the
anterior shoulder.
Episiotomy is repaired in the usual method.
32.
KIELLAND’S FORCEPS
Itcan be used in unrotated vertex or face
presentation.
The blades are named anterior and posterior.
The anterior blade is to be introduced first .
The blade is introduced along the sidewalls
of the pelvis and then rotated round the
fetal face to its anterior position.
The posterior blade is inserted directly under
guidance if right hand placed between head
and the hollow of the sacrum.
33.
CONT...
The occiputis rotated anteriorly.
The position is rechecked and traction is
applied.

















![Operative_obstetrics_Presentation3[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/operativeobstetricspresentation31-251210093149-f8512b7d-thumbnail.jpg?width=640&height=640&fit=bounds)






























