Downloaded 137 times


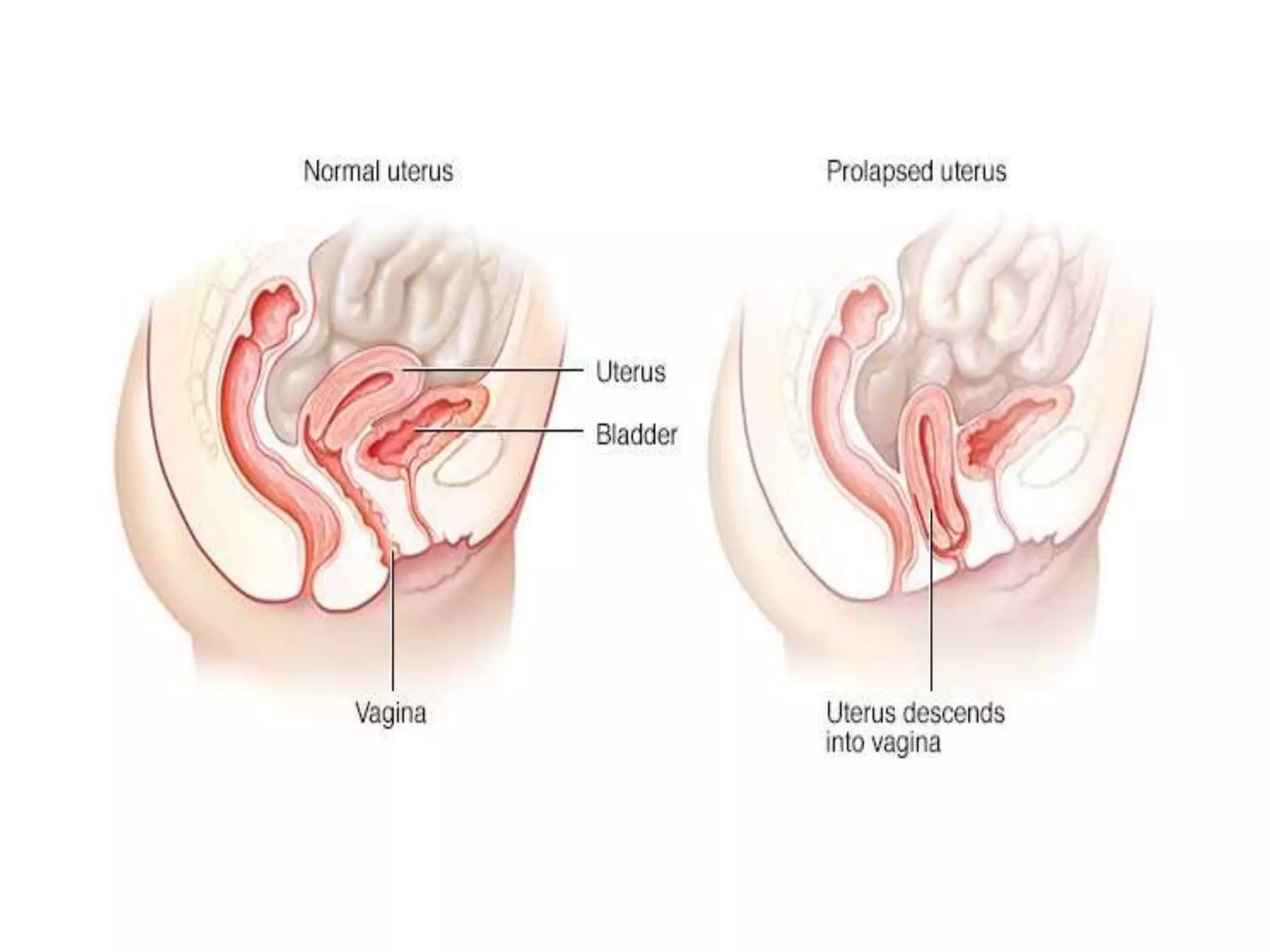























Genital prolapse is a common gynecological condition characterized by the descent of the vaginal wall or uterus, with varying degrees of severity. Pregnancy can occur in women with certain types of prolapse, but complications are likely when the cervix protrudes outside the vaginal opening. Treatment during pregnancy may involve repositioning the cervix and using a pessary, while the management of labor depends on the prolapse condition at that time.























































































