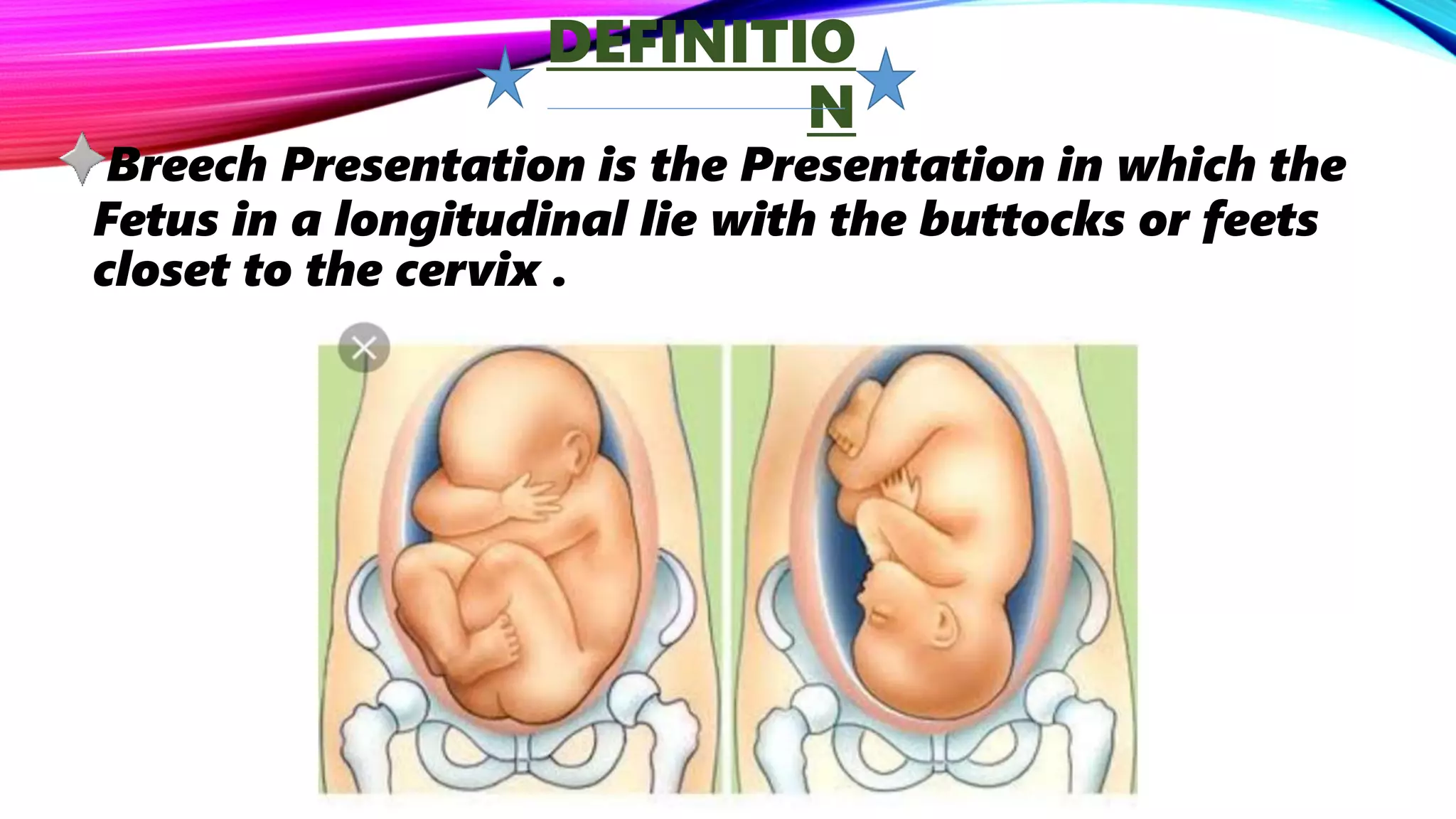
1) Breech presentation refers to when the fetus is positioned with the buttocks or feet closest to the cervix rather than the head. It occurs in 3-4% of pregnancies at term.
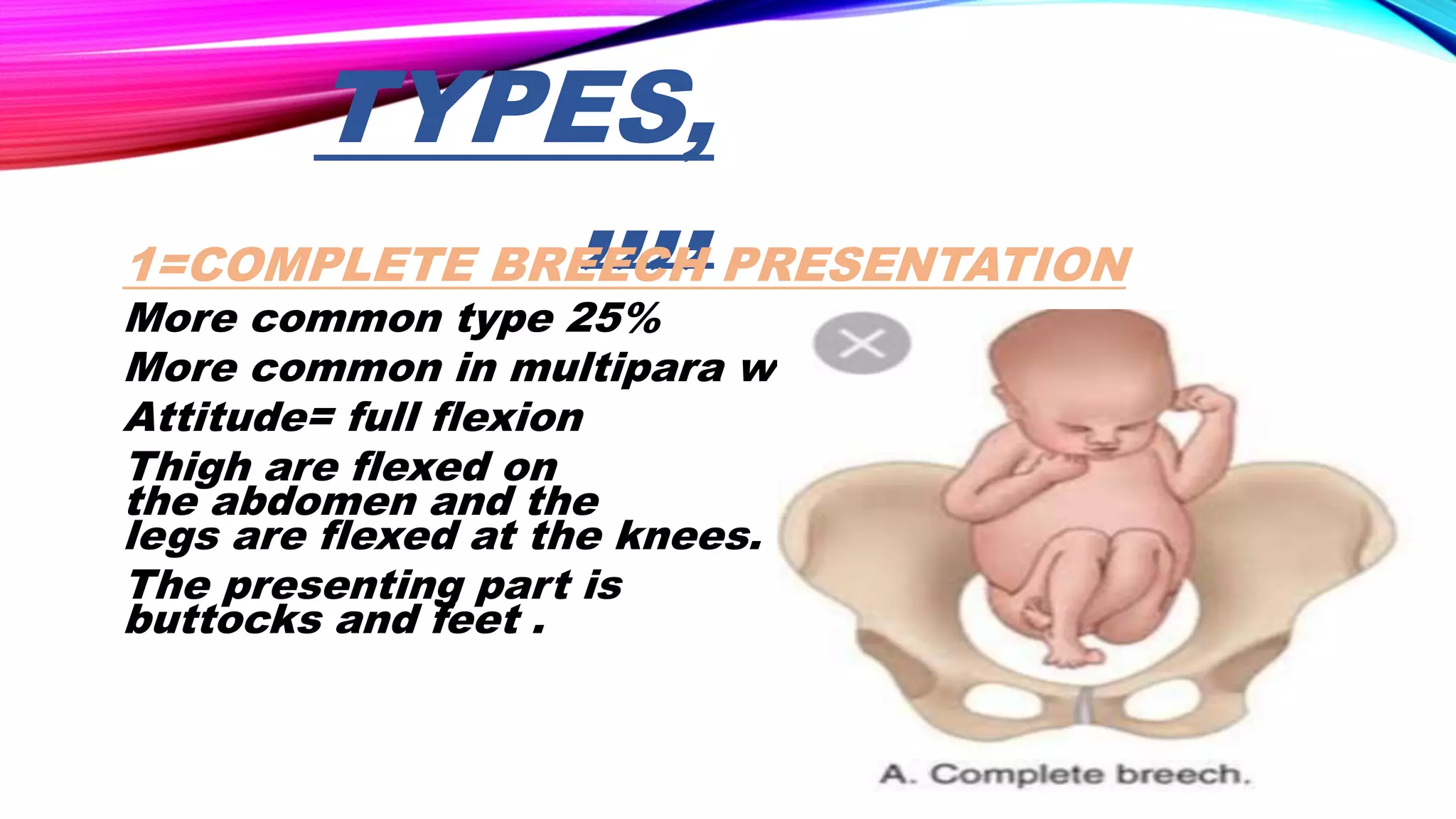
2) Risk factors for breech presentation include multiparity, uterine abnormalities, fetal factors like prematurity, and placental or amniotic fluid issues. There are different types including complete, frank, and footling breech.
3) Breech presentation is diagnosed through clinical examination including abdominal palpation and ultrasound. Management options include external cephalic version, planned c-section, or attempted vaginal breech delivery depending on the situation.




![ETIOLO
GY
1=MATERNAL FACTORS…….
[A]Grand Multipara
[B] Uterine Abnormalities[Bicorn ate septate
uterus]
[c] fibroid uterus
[D]Contracted Pelvis ,Multiple pregnancy
2=FETAL FACTORS…..
[A] Prematurity](https://image.slidesharecdn.com/rekharawat4year-190409072344/75/breech-presentation-8-2048.jpg)

![CONT.,,,,,
[B] Macrosomia
[c]Fetal Anomalies[Hydrocephalus ,
Anencephaly]
[E] Twin pregnancy
[F] Fetal death
[G] Extended legs](https://image.slidesharecdn.com/rekharawat4year-190409072344/75/breech-presentation-10-2048.jpg)
![CONT.,,,3= PLACENTAL,AMNIOTIC FLUID FACTORS…..
[A] Placenta Previa
[B] oligohydramnios
[C] Polyhydramnios
[D] Nuchal cord
[E] Short cord
[F] Trisomy](https://image.slidesharecdn.com/rekharawat4year-190409072344/75/breech-presentation-11-2048.jpg)

![CONT.,,,
2=FOOTLING BREECH[10-30%]
Both the thigh and legs are partially extended bringing
the legs to present at the brim.
*Foot is the lower part .
3=KNEE PRESENTATION
Thigh are extended but the knees are flexed ,bringing
the knees down to the brim](https://image.slidesharecdn.com/rekharawat4year-190409072344/75/breech-presentation-14-2048.jpg)







![MECHANISM OF
BREECH
• lie is longitudinal lie
• Attitude complete flexion
• Presentation breech
• Lt.sacro anterior position
• Denominator sacrum
• Presentig part anterior
Buttocks [left]](https://image.slidesharecdn.com/rekharawat4year-190409072344/75/breech-presentation-22-2048.jpg)