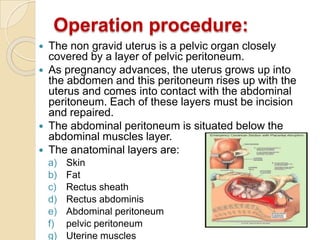
Caesarean section is a surgical procedure to deliver babies through incisions in the abdominal wall and uterus. The incidence of caesarean sections has steadily increased in recent decades due to improved safety and identification of risk factors. There are two main types - elective and emergency. Lower segment transverse incisions heal faster than classical incisions in the upper uterine segment. Post-operative care involves monitoring vitals, administering antibiotics and analgesics, encouraging early mobilization while avoiding complications like hemorrhage, infection, and thrombosis.