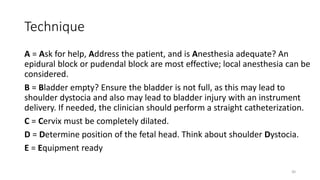
The document discusses operative vaginal delivery (OVD), detailing indications, prerequisites, contraindications, and performance techniques for vacuum and forceps delivery methods. It outlines the necessary preparations, instruments used, and potential risks associated with each method, as well as maternal and fetal complications. It also compares the advantages of forceps and vacuum delivery, presenting guidelines for safe application and management during the procedure.

































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)