Downloaded 247 times













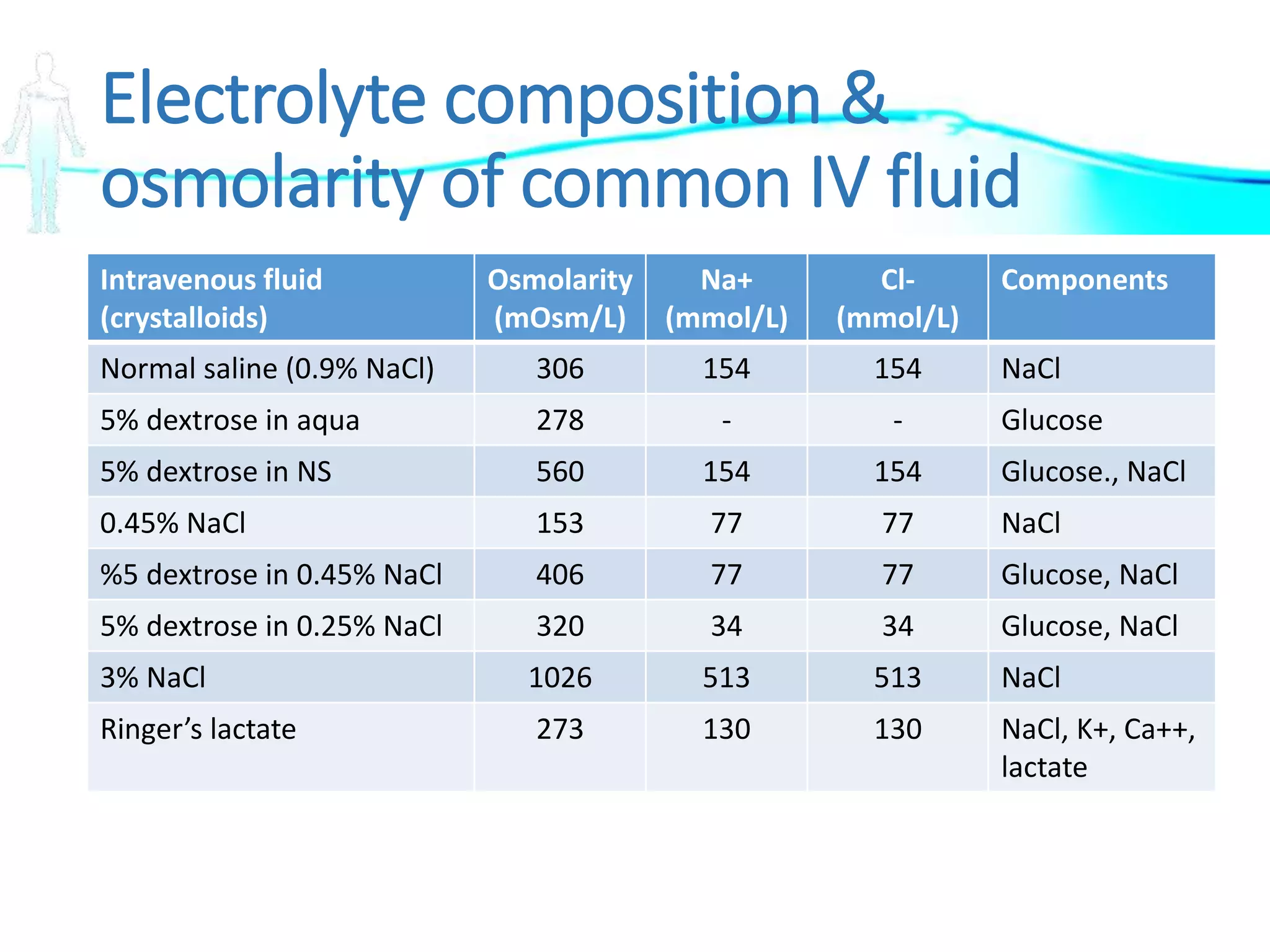


































































The document discusses the importance of fluid and electrolyte balance in pediatric gastroenterology. It covers concepts such as fluid compartments, types of intravenous fluid therapies (crystalloids and colloids), definitions of osmolality and tonicity, and specific situations for administering hypotonic, isotonic, and hypertonic solutions. Additionally, it addresses the regulation of potassium balance and treatments for potassium imbalances like hypokalemia and hyperkalemia.





















































































