Downloaded 94 times
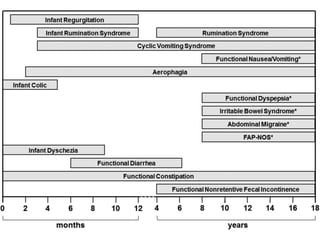
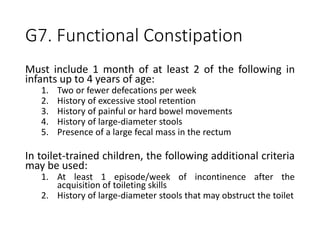
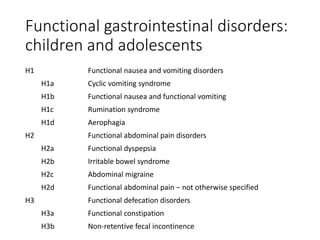

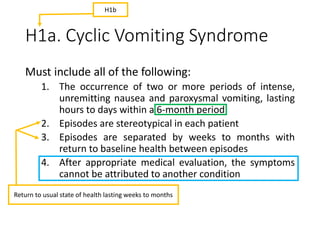
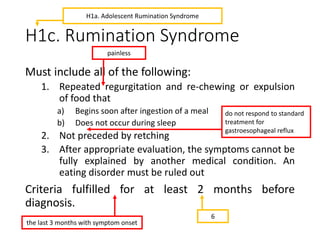
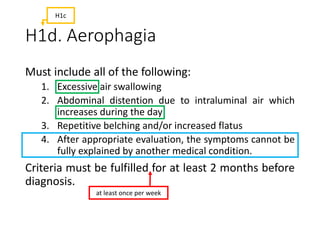
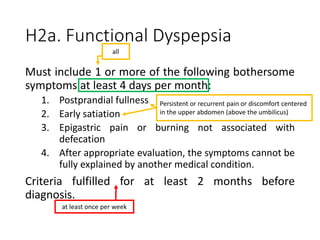
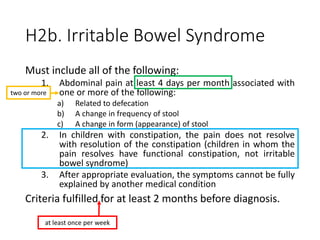
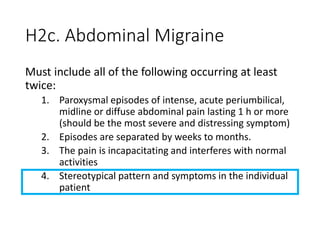
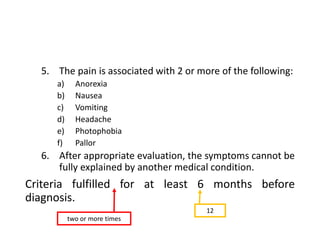
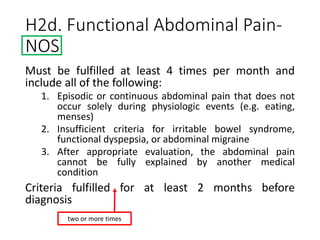


The document outlines the Paediatric Rome IV criteria developed for diagnosing functional gastrointestinal disorders in children and adolescents. It details various disorders such as infant colic, rumination syndrome, and irritable bowel syndrome, providing specific diagnostic criteria for each. The Rome IV criteria emphasize a shift from a physiologically based classification to a symptom-based approach to improve diagnosis and treatment globally.





















































































