Download to read offline
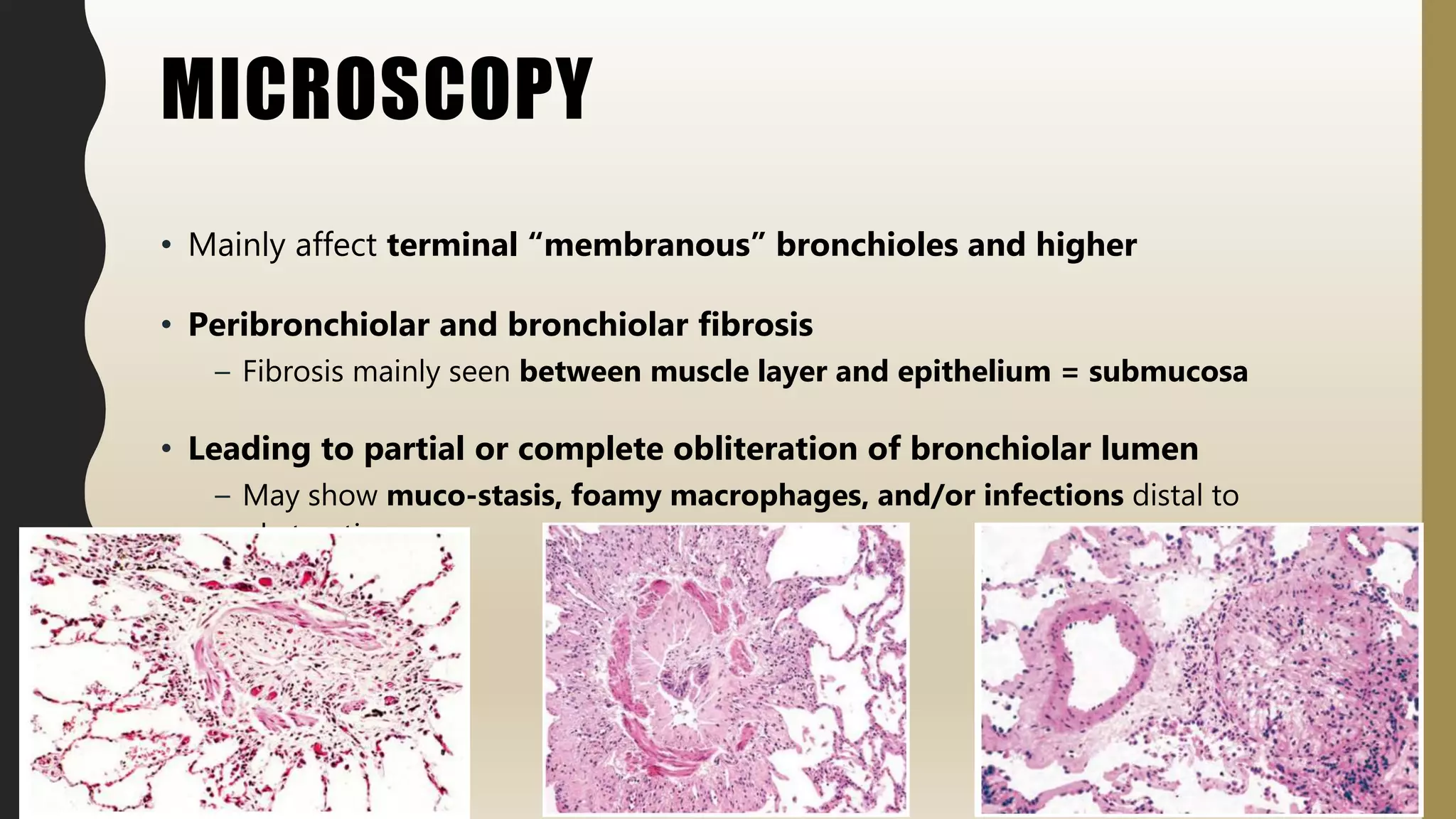
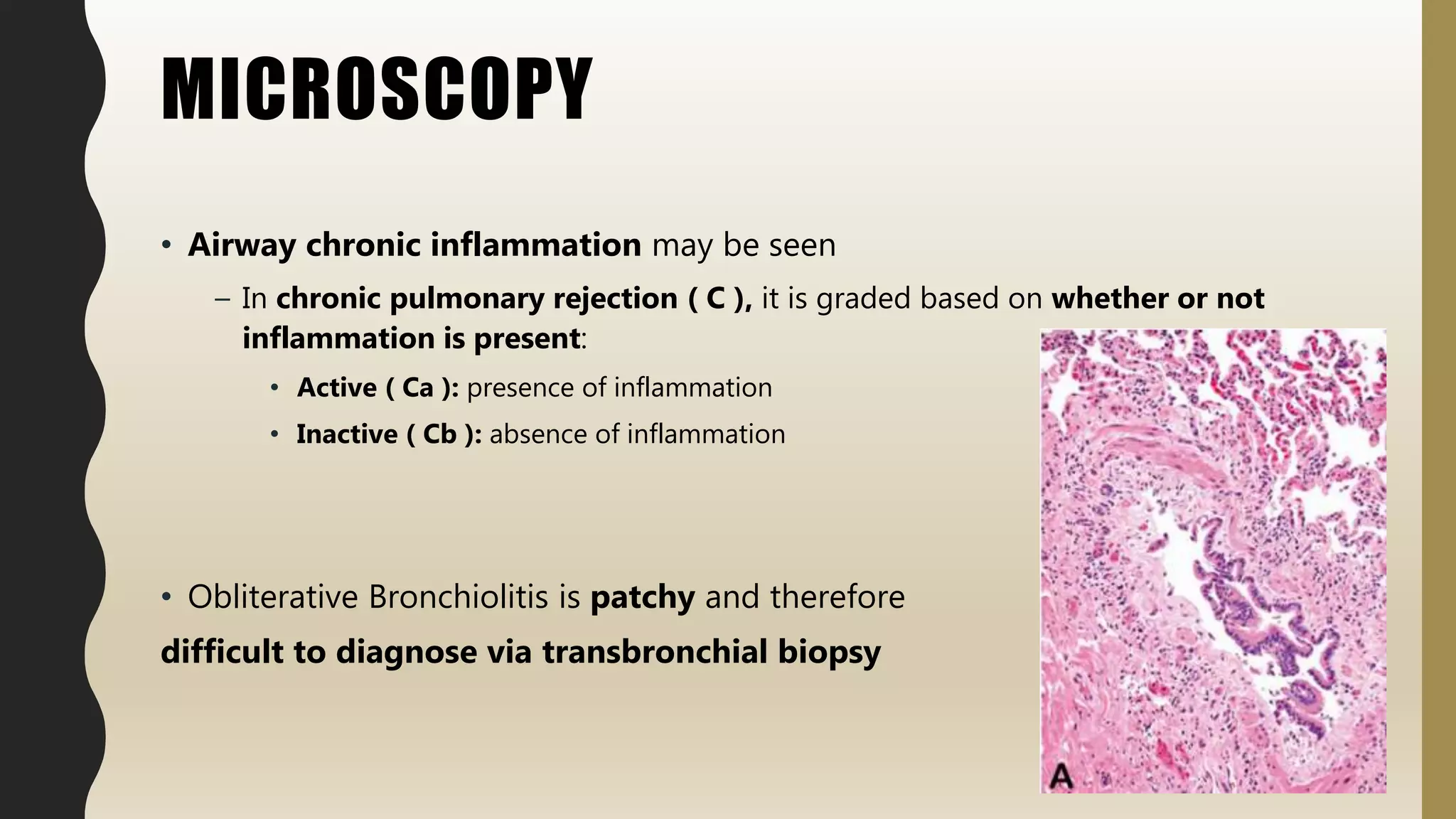
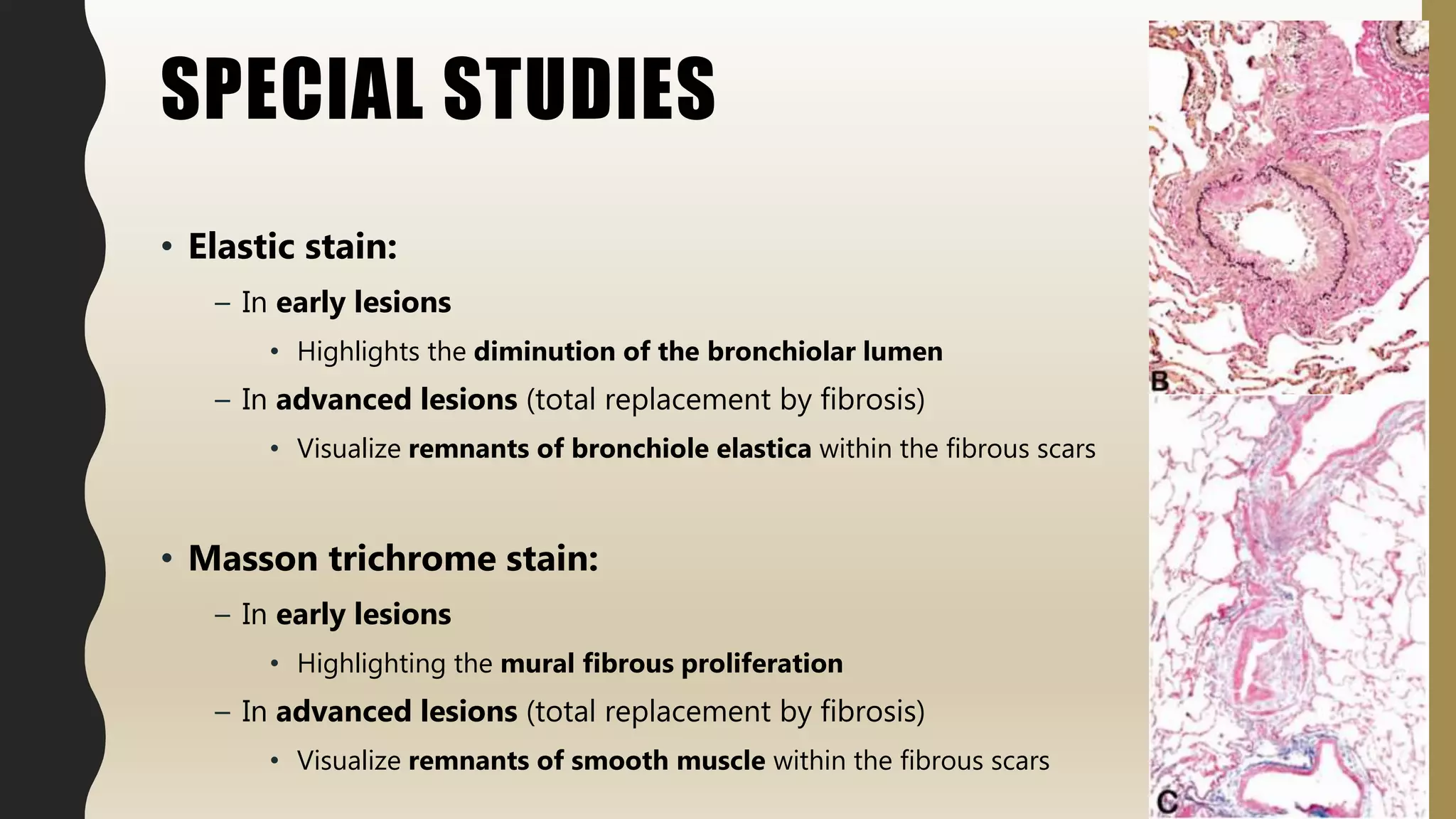
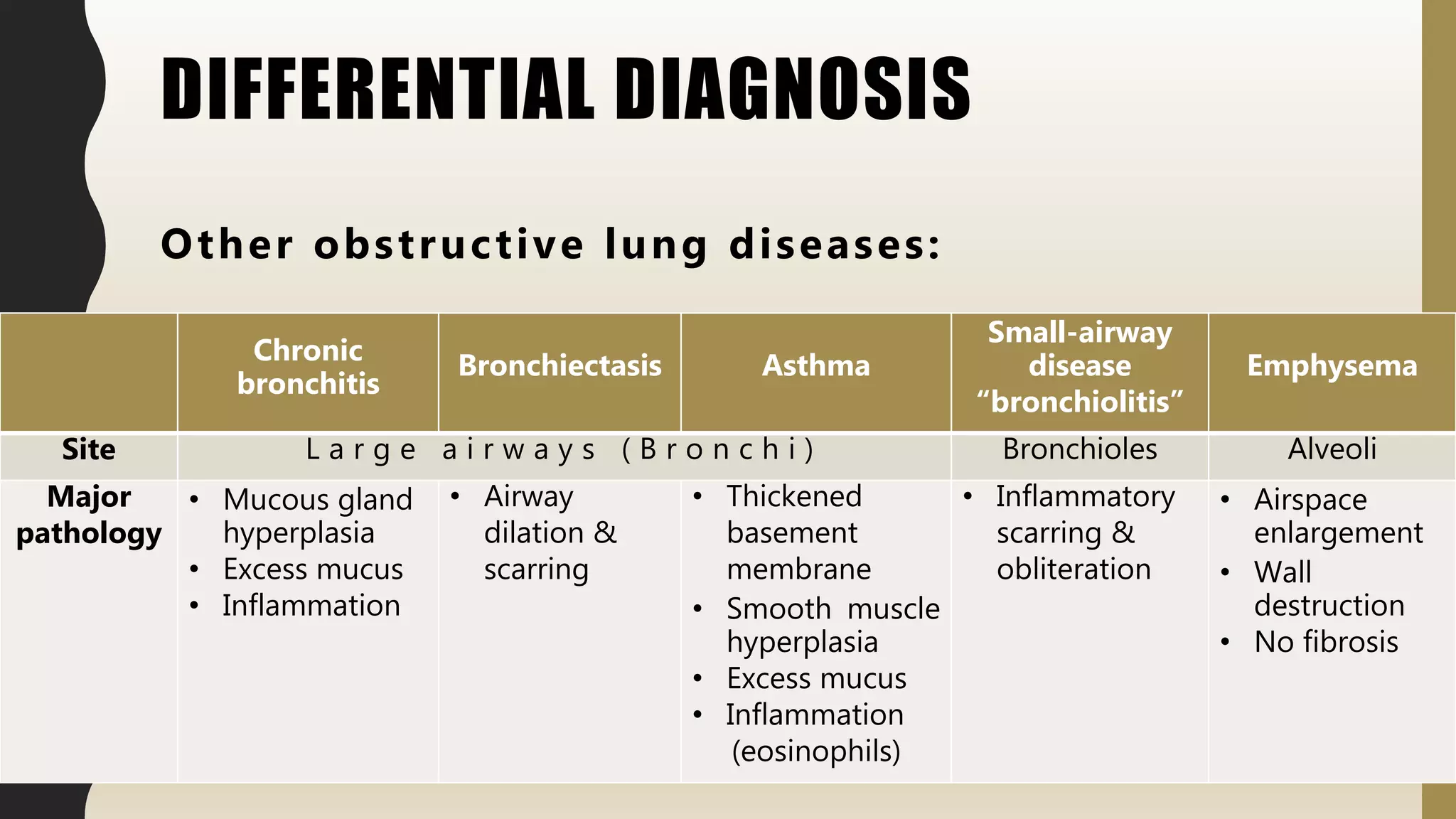
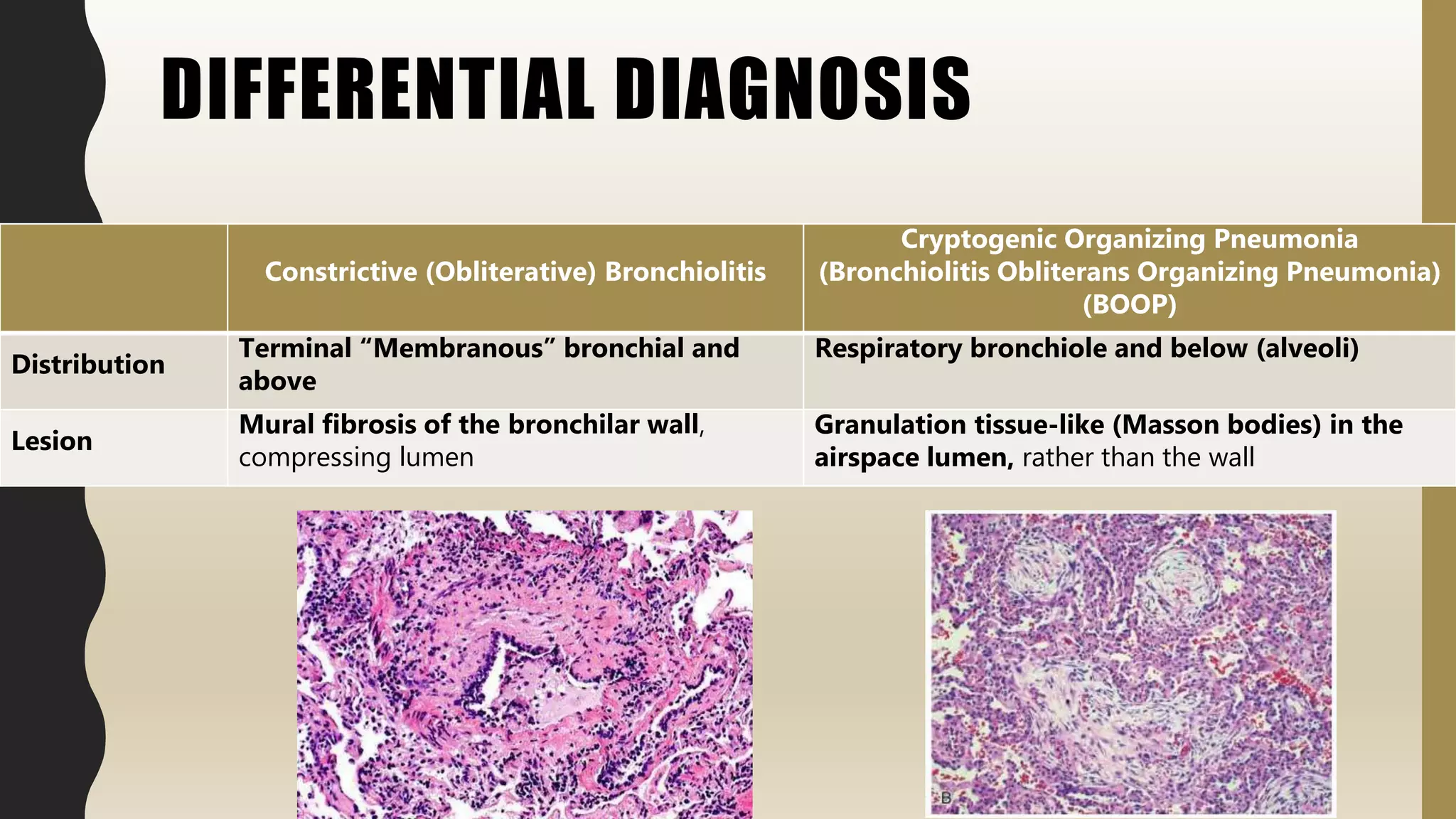

Constrictive bronchiolitis is an obstructive lung disease characterized by fibrosis and inflammation of the small airways leading to either partial or complete obstruction. It is commonly associated with lung transplantation, connective tissue diseases, certain drug toxicities, and viral infections. Microscopically it affects the terminal bronchioles and shows peribronchiolar fibrosis leading to bronchiolar lumen obliteration. It is differentiated from other obstructive lung diseases by its site of involvement in the small airways and pathology of mural fibrosis rather than airspace changes.























![EEG & Epilepsy syndromes report [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/e189c60d-77a3-4067-bdbe-fe484f4e5901-150602002311-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)































































