Downloaded 431 times
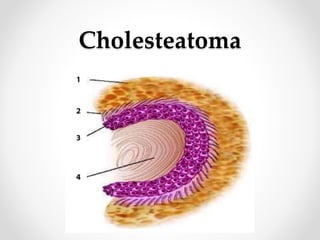

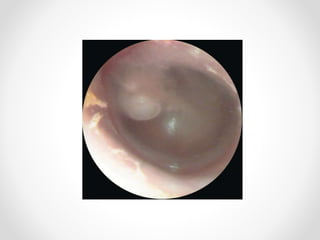
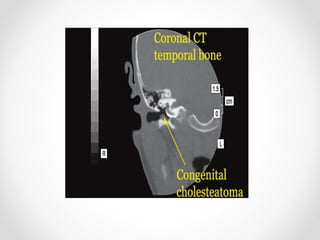


Cholesteatoma is a cyst-like structure in the middle ear filled with skin cells and debris. It can be congenital, arising from embryonic skin cell rests, or acquired through retraction of the eardrum or migration of skin cells through a perforated eardrum. The skin cells in the cholesteatoma produce enzymes that destroy the surrounding bone. Cholesteatoma is evaluated with examination, imaging, and hearing tests. Treatment involves surgery to remove the cholesteatoma and reconstruct the damaged bones.
































































































