Downloaded 15 times


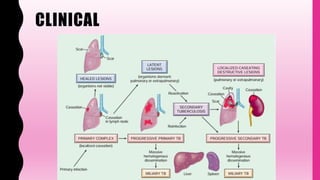
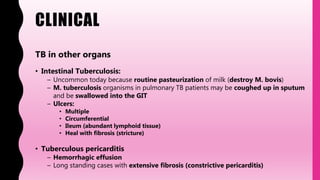





This document summarizes tuberculosis (TB), including: - It is caused by Mycobacterium tuberculosis and spreads through airborne droplets. It infects over 1 billion people worldwide and causes 1.5 million deaths annually. - Primary TB occurs in non-sensitized individuals, usually children, and involves subpleural lesions. Secondary TB occurs in previously sensitized adults and involves apical cavitation. - TB can affect any organ, causing lesions, lymphadenitis, meningitis. Advanced TB can cause destruction of organs. Diagnosis involves smears, cultures, skin tests, and molecular tests to detect the bacteria.























































































