














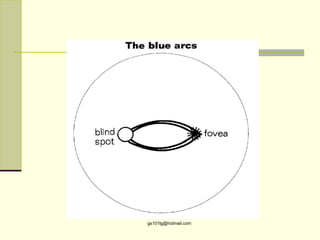

Entopic phenomena are visual sensations that originate from inside the eye. Some examples include seeing flashes of light when looking at a bright sky, which are caused by white blood cells moving through retinal blood vessels. Other entopic phenomena are produced by shadows cast on the retina from ocular structures and opacities, reflections and refractions of light within the eye, and pressure or movement of the eye. These phenomena are normal in most cases, but can sometimes indicate ocular issues like edema or retinal detachment. Understanding the various causes of entopic phenomena is important for eye health evaluations.












![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)