The document outlines a presentation on diagnostic cytopathology of serous effusions, focusing on various conditions such as benign disorders, mesothelioma, and metastatic carcinomas. It discusses the importance of careful evaluation of cytology samples, potential diagnostic pitfalls, and the relevant characteristics of various cell types observed in effusions. Additionally, it emphasizes the significance of clinical history in interpreting cytology findings for accurate diagnosis.
![1 Diagnostic Cytopathology of Serous Effusions Session II ( 8.45-9.30 ) To view this session on web copy-paste the following URL into your browser: http://www.slideshare.net/vshidham/02-presentations-ii-vs-14-4-mb-3-30-08 Vinod B. Shidham , MD, FRCPath, FIAC Professor Executive editor & coeditor-in-chief, CytoJournal ( www.cytojournal.com ) Department of Pathology Medical College of Wisconsin 9200 W Wisconsin Av, Milwaukee, WI 53226, USA [email_address] 2008 Wisconsin Society of Cytology SPRING MEETING, 40TH ANNIVERSARY Holiday Inn – Riverwalk, Neenah, WI Saturday, April 19, 2008 (7.30 to 3.30)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-1-320.jpg)
![1 Diagnostic Cytopathology of Serous Effusions Session II ( 8.45-9.30 ) To view this session on web copy-paste the following URL into your browser: http://www.slideshare.net/vshidham/02-presentations-ii-vs-14-4-mb-3-30-08 Vinod B. Shidham , MD, FRCPath, FIAC Professor Executive editor & coeditor-in-chief, CytoJournal ( www.cytojournal.com ) Department of Pathology Medical College of Wisconsin 9200 W Wisconsin Av, Milwaukee, WI 53226, USA [email_address] 2008 Wisconsin Society of Cytology SPRING MEETING, 40TH ANNIVERSARY Holiday Inn – Riverwalk, Neenah, WI Saturday, April 19, 2008 (7.30 to 3.30)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/75/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-1-2048.jpg)
![Benign conditions with/without specific cellular patterns (continued) Reactive mesothelial cells in clusters (ascitic fluid). Mixed with chronic inflammatory cells within the groups and between the mesothelial cells in the background. [Papanicolaou stained ThinPrep preparation (100x Zoomed)]. 6](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-7-320.jpg)
![Benign conditions with/without specific cellular patterns (continued) Reactive mesothelial cells in clusters mixed with chronic inflammatory cells, mostly mature lymphocytes (ascitic fluid). This consult case was initially misinterpreted as positive for malignant cells. Extensive search for primary was negative. [Papanicolaou stained ThinPrep preparation (100x Zoomed)]. 7](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-8-320.jpg)
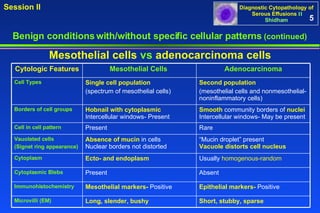
![Benign conditions with/without specific cellular patterns (continued) A thin rim between nuclear border and cell border (1) is seen in mesothelial cells. In comparison, the nuclear border touches the cell border of adenoca cells without a significant cytoplasmic rim (2). [Papanicolaou stained SurePath TM Preparation (b,c,e,f, 100XZoomed)]. Mesothelial cells (a,b,&c) versus adenocarcinoma cells (d,e,&f) with eccentric nuclei . 9 2 2 2 f e d Adenocarcinoma 1 1 1 a c b Mesothelial](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-10-320.jpg)
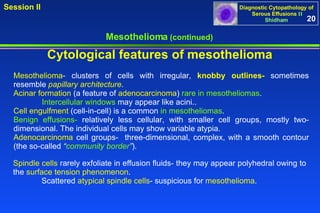


![Mesothelioma (continued) Cytological features of mesothelioma Malignant epithelioid mesothelioma (pleural fluid). Mesothelioma cells show numerous large three dimensional groups of cells. The individual mesothelioma cells hardly show any variation from reactive mesothelial cells without remarkable features of malignancy. The mesothelioma cells like reactive mesothelial cells show two zone staining (red arrow 1) with peripheral vacuolation (blue arrow 2). [a-h, Papanicolaou stained ThinPrep preparation (a,b, 20X; c, 100X; d-h, 100XZoomed)]. 24 1 2 a b c e f g h d](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-25-320.jpg)

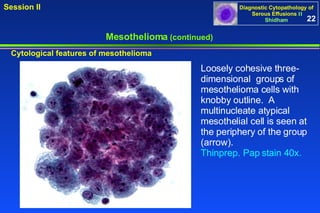
![Mesothelioma (continued) Peritoneal fluid, Deciduoid mesothelioma . Dyscohesive scattered single atypical enlarged cells Pap stain 10X. [Courtesy Dr. Bernard Naylor]. Cytological features of mesothelioma 27](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-28-320.jpg)
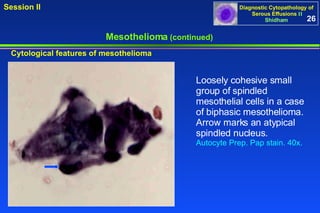
![Mesothelioma (continued) Peritoneal fluid, Deciduoid mesothelioma. Enlarged malignant cells with a binucleate form, and glassy cytoplasm. Nuclei are vesicular with prominent nucleoli. Scattered smaller atypical mesothelial cells are present in the background. Pap stain 40X [Courtesy Dr. Bernard Naylor]. Cytological features of mesothelioma 28](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-29-320.jpg)

![Metastatic adenocarcinoma- NOS , (peritoneal fluid). Cohesive groups of cells in papillary configurations show eccentrically placed nuclei touching the periphery of cells (arrows in b,c,f). The cells in such groups are difficult to study at lower magnification (a,b). However, the cell morphology in such groups can be observed at the periphery, especially under higher magnification (arrow in b). Some groups show gland-like spaces (arrowheads in d,e,f). [a-c: Papanicolaou stained SurePath preparation; d-f: Diff-Quik stained Cytospin preparation. (a, 10X; b, 40X; c, 100XZoomed; d, 10X; e, 40X; f, 100XZoomed)]. 36 Characteristic features of some specific primary sites a b c d e f](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-37-320.jpg)
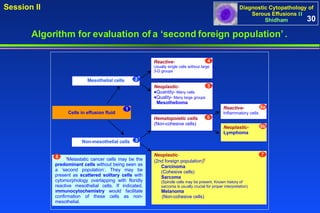
![a b c d e f w 2 1 Metastatic poorly differentiated adenocarcinoma of lung, (pleural fluid). The Diff-Quik stained preparation demonstrates reactive mesothelial cells (arrowhead 1 in a) mixed with a ‘second population’ of cohesive groups of cells (arrow 2 in a) with eccentric nuclei that touch the periphery of the carcinoma cells (arrowheads in b,c,f). Some cells are less cohesive with nearby small groups or solitary carcinoma cells (arrows in d,e,f). Occasional intercellular spaces, resembling mesothelial window, are present (arrowhead w in c). The patient had poorly differentiated adenocarcinoma of lung. [a-c: Diff-Quik stained Cytospin preparation, d-f: Papanicolaou stained SurePath preparation. (a, 10X; b,c, 100X; d, 10X; e,f, 100X)]. 37 Characteristic features of some specific primary sites (continued)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-38-320.jpg)
![a c d g h e f i j RM b RM c g j i h d f e Ly NC RM nm nm NC Metastatic small cell carcinoma, (pleural fluid). Cancer cells (a,b) are present as solitary cells (c,d), small groups (g,h,i), and large groups (b & j). The cells are small with high nucleocytoplasmic ratios (c,d,g,h.i). The nuclei are hyperchromatic with salt and pepper chromatin (c,d,i). Solitary cancer cells (NC) (c,d) resemble lymphocytes (blue arrow Ly in f) and may be misinterpreted as lymphoma, especially in PAP stained preparations. However, the presence of cohesive groups (g,h,i,j) with various patterns, including Indian-file pattern (g), typify carcinoma. The nuclear molding (arrows nm in g & i) distinguishes them from other poorly differentiated carcinomas. Mitotic figures (arrowhead in e) and apoptotic cancer cells (arrowheads in d,f,h) are also present. Rare reactive mesothelial cells (blue arrows RM in a,b,e) are present with a few chronic inflammatory cells (blue arrow Ly in f) in the background. Immunostained cell block sections showed immunoreactivity for neuroendocrine immunomarkers (chromogranin, synaptophysin, and CD56). The patient had poorly differentiated small cell carcinoma of lung. (NC, neoplastic cell; RM, reactive mesothelial cell, nm, nuclear molding, Ly, lymphocyte) [a-j: Papanicolaou stained SurePath preparation. (a-b, 100X; c-j, 100XZoomed)]. 38 Characteristic features of some specific primary sites (continued)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-39-320.jpg)
![a b c d e f g h RM NC NC NC RM TTF-1 Metastatic bronchioloalveolar cell carcinoma of lung , (pleural fluid). Cellular specimen (a) shows three dimensional groups of carcinoma cells (arrowheads in a-f) mixed with reactive mesothelial cells (blue arrow RM in f,g). The two populations are demonstrated more distinctly with the DQ stain (f,g) than with the PAP stain (a-e). However, the morphological details of individual neoplastic cells are superior in the PAP stain (a-e), especially under higher magnification (c-e). The individual cells show features of well differentiated adenocarcinoma (red arrows NC in d,e,g). Although, usually not conspicuous, some of the carcinoma cells have prominent nucleoli (d,e). The neoplastic cells demonstrate nuclear immunoreactivity for TTF-1 (arrowheads in h) consistent with a lung primary. The patient had bronchioloalveolar cell carcinoma of lung. (NC, neoplastic cell; RM, reactive mesothelial cell; TTF-1 Thyroid transcription factor- 1) [a-e: Papanicolaou stained SurePath preparation; f-g: Diff-Quik stained Cytospin preparation; h: Immunostained cell-block section. (a, 10X; b, 40X; c, 100X; d-e, 100XZoomed; f, 40X; g, 100X; h, 40X)]. 39 Characteristic features of some specific primary sites (continued)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-40-320.jpg)
![Metastatic mammary carcinoma, (pleural fluid). a-g: Proliferation spheres (red arrows NC) with mostly reactive mesothelial cells (blue arrows RM) and inflammatory cells in the background, clearly separated out in the immunostained cell-block sections (a,e). The reactive mesothelial cells (blue arrows RM) stand out distinctly from the neoplastic cells (red arrow NC) in the DQ stain. However, the reactive mesothelial cells in the PAP stain (blue arrows in g) are difficult to distinguish from neoplastic cells (compare with case in h-j). h-j: A different patient with metastatic mammary carcinoma. The effusion predominantly contains solitary adenocarcinoma cells, as highlighted by the BerEP4 immunostained section (red arrows NC in h). The carcinoma cells (red arrows NC in j) can be distinguished easily from reactive mesothelial cells (blue arrow RM in j) in the DQ stain (j), but not in the PAP stain (i). A mitotic figure is present (blue arrow MF in i). Note the resemblance of reactive mesothelial cells in f & g to neoplastic cells in i. Without the help of DQ stain and immunocytochemistry, such fluids, with predominantly one type of cell population, may easily be misinterpreted. [a,e,h: Immunostained cell-block sections; f,g,i: Papanicolaou (PAP) stained SurePath preparation; b,c,d,,j: Diff-Quik (DQ) stained Cytospin preparation. (a, 40X; b, 100X; c,d, 100XZoomed; e, 40X; f, 100X; g, 100XZoomed; h, 40XZoomed; i, 100X; j, 100XZoomed)]. 40 Characteristic features of some specific primary sites (continued) Calretinin RM NC BerEP4 RM NC NC BerEP4 NC NC NC RM g i h f e c a j b d MF RM NC RM RM RM RM RM NC RM](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-41-320.jpg)
![Metastatic adenocarcinoma of colon, (peritoneal fluid). Cohesive groups of cells (a) show high nucleocytoplasmic ratios and eccentric nuclei touching the periphery of the cell (arrow in b). Some adenocarcinoma cells show cytoplasmic vacuoles containing mucin (arrowhead in the inset of b). The cell groups in papillary configurations are difficult to study at lower magnification (c). Peripheral palisading is better observed under higher magnification (d). The patient had colonic adenocarcinoma. [a,b: Diff-Quik (DQ) stained Cytospin preparation, c-d: Papanicolaou (PAP) stained SurePath preparation. (a, 40X; b, 100X; c, 40X; d, 100)]. 41 Characteristic features of some specific primary sites (continued) a b c d](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-42-320.jpg)
![Metastatic gastric adenocarcinoma, (peritoneal fluid). The specimen contained a predominance of solitary neoplastic cells (red arrows a,d) with rare reactive mesothelial cells (blue arrow RM in a). Most of the cancer cells have eccentric nuclei touching the periphery of the cells (a,b,c,d). The reactive mesothelial cells (blue arrow RM) are identifiable more easily in the Diff-Quik stained (a) than in the PAP stained (c) preparation. The solitary carcinoma cells may be misinterpreted as high-grade lymphoma cells, especially in PAP stained preparations (c,d). Apoptotic cancer cells (yellow arrow ‘e’ in c) and mitotic figures (yellow arrow ‘f’ in c) are also present. The predominance of solitary neoplastic cells (a-j) is confirmed in the HE stained (g & h) and BerEP4 (i) immunostained cell-block sections. A few CK 7 immunoreactive mesothelial cells, as intrinsic positive control, are present amongst many neoplastic cells (j). Although, the adenocarcinoma cells in this case were non-immunoreactive for CK 7 (j), a significant proportion of gastric adenocarcinomas are immunoreactive for CK 7. The patient had linitis plastica type diffuse anaplastic gastric adenocarcinoma. (AP, apoptotic cancer cell; CK 7, cytokeratin 7; MF, mitotic figure; NC, neoplastic cell; RM, reactive mesothelial cell) [a-b: Diff-Quik (DQ) stained Cytospin preparation; c-f: Papanicolaou (PAP) stained SurePath preparation; g,h: HE stained cell-block section; i,j: Immunostained cell-block sections. (a, 100X; b, 100XZoomed; c, 100X; d-f, 100XZoomed; g, 40X; h-j 100X)]. 42 Characteristic features of some specific primary sites (continued) a c b d g h e f i j RM d f e b BerEP4 CK 7 NC NC AP MF](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-43-320.jpg)
![Metastatic pancreatic adenocarcinoma, (peritoneal fluid). The neoplastic cells (NC) are as loosely cohesive groups (a) or as solitary cells (b,e) with eccentric nuclei. PAP stained preparations facilitate evaluation of cellular details in cohesive groups (c & d). A few cell groups show gland-like structures (arrow in d). ‘Second population’ (arrows in f,g,&h) of neoplastic cells is highlighted distinctly in immunostained cell-block sections f through h (immunoreactive for BerEP4 in f, non-immunoreactive for vimentin in g and calretinin in h). As inbuilt corresponding positive controls, inflammatory and reactive mesothelial cells (arrowhead in g) are immunoreactive for vimentin and reactive mesothelial cells (arrowhead RM in h) are immunoreactive for calretinin. The patient had pancreatic adenocarcinoma. (NC, neoplastic cell; RM, reactive mesothelial cell) [a-b: Diff-Quik (DQ) stained Cytospin preparation; c-e: Papanicolaou (PAP) stained SurePath preparation; f-h: Immunostained cell-block sections. (a-e, 100X; f-h, 40X)]. 43 Characteristic features of some specific primary sites (continued) BerEP4 f d e c b a bi bii vimentin NC NC NC NC Calretinin RM g h](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-44-320.jpg)
![Metastatic ovarian serous papillary cystadenocarcinoma, (peritoneal fluid). Psammoma bodies (red arrows PSM in a.b,c,e,f,i) are present, isolated and in association with papillary clusters (d,f) of adenocarcinoma cells without stromal cores (g,h). Some carcinoma cells show degenerative vacuoles (blue arrows VAC in h), which should not be misinterpreted as mucinous. Some apoptotic neoplastic cells (blue arrow AP in i) are present. (AP, apoptotic cancer cell; NC, neoplastic cell; PSM, psammoma body; VAC, vacuole) [a-i: Papanicolaou (PAP) stained SurePath preparation. (a, 20X; b, 40X; c-e, 100X, f-i , 100XZoomed)]. 44 Characteristic features of some specific primary sites (continued) a b c d e f g h i PSM VAC PSM PSM PSM PSM AP PSM VAC NC](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-45-320.jpg)
![Primary peritoneal carcinoma, (peritoneal fluid). The specimen shows a predominance of groups of adenocarcinoma cells in papillary configurations (a,d) without stromal cores (g). Solitary neoplastic cells (red arrows NC in a,b,d,e) are easily distinguished from the rare reactive mesothelial cells (blue arrowheads RM in a,c,d,e). However, in PAP stained preparation (d), reactive mesothelial cells (arrowhead RM in e) have significant morphological overlap with neoplastic cells (red arrows NC in d & e). Mitotic figures (yellow arrow MF in a) and apoptotic cells (yellow arrows AP in d,f) are present concurrently. Some cells show degenerative vacuolation (a,b). These vacuoles may resemble secretory vacuoles and lead to misinterpretation of mucinous adenocarcinoma. The cancer cells do not show nuclear immunoreactivity for calretinin (h), but they are immunoreactive for BerEP4 (i). The neoplastic cells show nuclear (and cytoplasmic) immunoreactivity for WT-1(j). The patient had ascites with diffuse peritoneal involvement with omental caking. The ovaries were not enlarged. (AP, apoptotic cancer cell; MF, mitotic figure; NC, neoplastic cell; RM, reactive mesothelial cell) [a-c: Diff-Quik (DQ) stained Cytospin preparation; d-f: Papanicolaou (PAP) stained SurePath preparation; g: HE stained cell-block section; h-j: Immunostained cell-block sections. (a, 100X; b,c, 100XZoomed; d, 100X; e,f, 100XZoomed; h-j, 100X)]. 45 Characteristic features of some specific primary sites (continued) a d b c g h e f i j WT-1 BerEP4 Calret c b RM NC AP e f RM NC AP MF NC RM NC NC RM NC](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-46-320.jpg)
![a b c d Metastatic ovarian mucinous cystadenocarcinoma, (peritoneal fluid). Cohesive groups of neoplastic cells with high nucleocytoplasmic ratios and eccentric nuclei touching the periphery of the cells (arrow in b) are present. Some carcinoma cells have cytoplasmic vacuoles (a,b). The cell groups in papillary configurations are difficult to study at lower magnification (c). However, the cell morphology in such groups can be observed at the periphery of the papillation, especially under higher magnification (arrow in d). The patient had ovarian mucinous cystadenocarcinoma. [a,b: Diff-Quik (DQ) stained Cytospin preparation; c,d: Papanicolaou (PAP) stained SurePath preparation. (a, 40X; b, 100X; c, 40X; d, 100X)]. 46 Characteristic features of some specific primary sites (continued)](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-47-320.jpg)
![Metastatic ovarian adenocarcinoma, (peritoneal fluid). The neoplastic cells show an Indian file pattern. This arrangement is not specific for particular carcinoma (Ref 14); in addition to metastatic mammary carcinoma and small cell carcinoma of lung (see Figure 9.3a,b,g), this pattern may be seen in other non-small cell carcinomas, as in this case with metastatic ovarian adenocarcinoma. [a: Papanicolaou (PAP) stained SurePath preparation; b: Diff-Quik (DQ) stained Cytospin preparation. (a-b, 100X)]. 47 Characteristic features of some specific primary sites (continued) a b](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-48-320.jpg)
![Metastatic carcinoma of endometrium, (pleural fluid). Papillary-like cohesive groups (blue arrow in a) of columnar cells (red arrow in d). The patient had endometrial carcinoma of endometrioid type. [a-d: Papanicolaou (PAP) stained SurePath preparation. (a, 10X; b, 40X; c,d, 100X)]. 48 Characteristic features of some specific primary sites (continued) a b c d](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-49-320.jpg)
![Metastatic prostatic adenocarcinoma, (peritoneal fluid). Cohesive small groups of cancer cells (red arrows in a,e,f,i,j) with mostly eccentric nuclei touching the periphery of the cells are present with some solitary cancer cells (red arrows NC in a,,c,d,f,g,h). Reactive mesothelial cells (blue arrows RM in a,b) are more easily and distinctly identifiable in DQ stained (a) than in PAP stained (f) preparations. Most cancer cells were poorly cohesive, manifested by the presence of small groups (e,i,j) or solitary cells (c,d,g,h). Some cells show vacuolation (f,g,h,i,j) which may be in vitro degenerative or functional with secretion. The patient had prostatic adenocarcinoma with colonic metastasis. The primary tumor also showed a few vacuolated cancer cells in tissue sections. (NC, neoplastic cell; RM, reactive mesothelial cell) [a-e: Diff-Quik (DQ) stained Cytospin preparation; f-j: Papanicolaou (PAP) stained SurePath preparation. (a, 100X; b-e, 100XZoomed; f, 100X; g-j, 100XZoomed)]. 49 Characteristic features of some specific primary sites (continued) RM RM RM a f b c d e g h i j RM RM NC NC NC NC NC NC](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-50-320.jpg)
![Metastatic papillary carcinoma of thyroid, (pleural fluid). ‘ Second population’ of cohesive papillary groups (red arrows NC in b,e,f) of cells associated with Psammoma bodies with concentric lamination (red arrow PSM in g2,h2’) are seen amongst a few reactive mesothelial cells (blue arrows RM in b,i). d1, single tumor cells with eccentric nucleus touching the periphery (blue arrow) DQ stained preparation. d2, single cells may have cytoplasmic vacuole with colloid (arrowhead) in DQ stained preparation. j1, single tumor cells with eccentric nucleus touching the periphery in PAP stained preparation. j2, compare with reactive mesothelial cell (binucleate) with central nuclei in j1 in PAP stained preparation. The patient had papillary carcinoma of thyroid. [NC, neoplastic cell(s); PSM, psammoma body; RM, reactive mesothelial cell(s)] [a-d: Diff-Quik (DQ) stained Cytospin preparation; e-j: Papanicolaou (PAP) stained SurePath preparation. (a, 40X; b,c, 100X; d1,d2, 100XZoomed; e, 10X; f, 40X; g1,g2,h1,h2,i, 100X; j1,j2, 100XZoomed)]. 50 Characteristic features of some specific primary sites (continued) a b c e g1 f d1 d2 g2 Second focus of ‘h1’ ( bright light) h1 h2 i j1 j2 NC RM NC RM NC NC Second focus of ‘g1’ ( bright light) PSM PSM](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-51-320.jpg)
![Metastatic cholangiocarcinoma, (peritoneal fluid). Cancer cells (red arrows in a,h) are present mostly as solitary cells with eccentric nuclei touching the periphery of the cells (b,d,i,k,l) with occasional loosely cohesive groups of cancer cells (a,f) and reactive mesothelial cells (c,e,j and arrowheads in a,h). A few cells show cytoplasmic vacuoles (i) with secretion (yellow arrow in l) which is positive for mucicarmine in cell-block section (n). Some apoptotic cancer cells (yellow arrow AP) are also present (g,m). The morphological features overlap those of other mucinous adenocarcinomas. The patient had cholangiocarcinoma with a mucinous pattern. (AP, apoptotic cancer cell; NC, neoplastic cell; RM, reactive mesothelial cell) [a-g: Diff-Quik stained Cytospin preparation; h-m: Papanicolaou stained SurePath preparation; n: Mucicarmine stained cell block section. (a, 100X; b-g, 100XZoomed; h, 100X; i-m, 100XZoomed); n, 100XZoomed)]. 51 Characteristic features of some specific primary sites (continued) a b h c d e i k b c d e l k i m g l j f f g m n j AP NC RM NC RM NC RM NC AP](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-52-320.jpg)
![Metastatic non-epithelial neoplasms (continued) Desmoplastic small round cell tumor (DSRCT) (peritoneal fluid). Dyshesive clusters of small round tumor cells showing rosette-like features (FNAB). DSRCT effusion exhibiting high cellularity. The tumor cells showed nuclear immunoreactivity for WT1. [ With thanks from the article in ‘open access’ cytopathology journal: Granja NM et al CytoJournal 2005, 2:6 Free full text at- http://www.cytojournal.com/content/pdf/1742-6413-2-6.pdf ] 57](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-58-320.jpg)
![Thank you Milwaukee Art Museum [email_address] End Diagnostic Cytopathology of Serous Effusions II](https://image.slidesharecdn.com/02-presentations-ii-vs-14-4-mb-3-30-08-1206896463191215-4/85/02-Presentations-Ii-Vs-14-4-Mb-3-30-08-66-320.jpg)

























































































