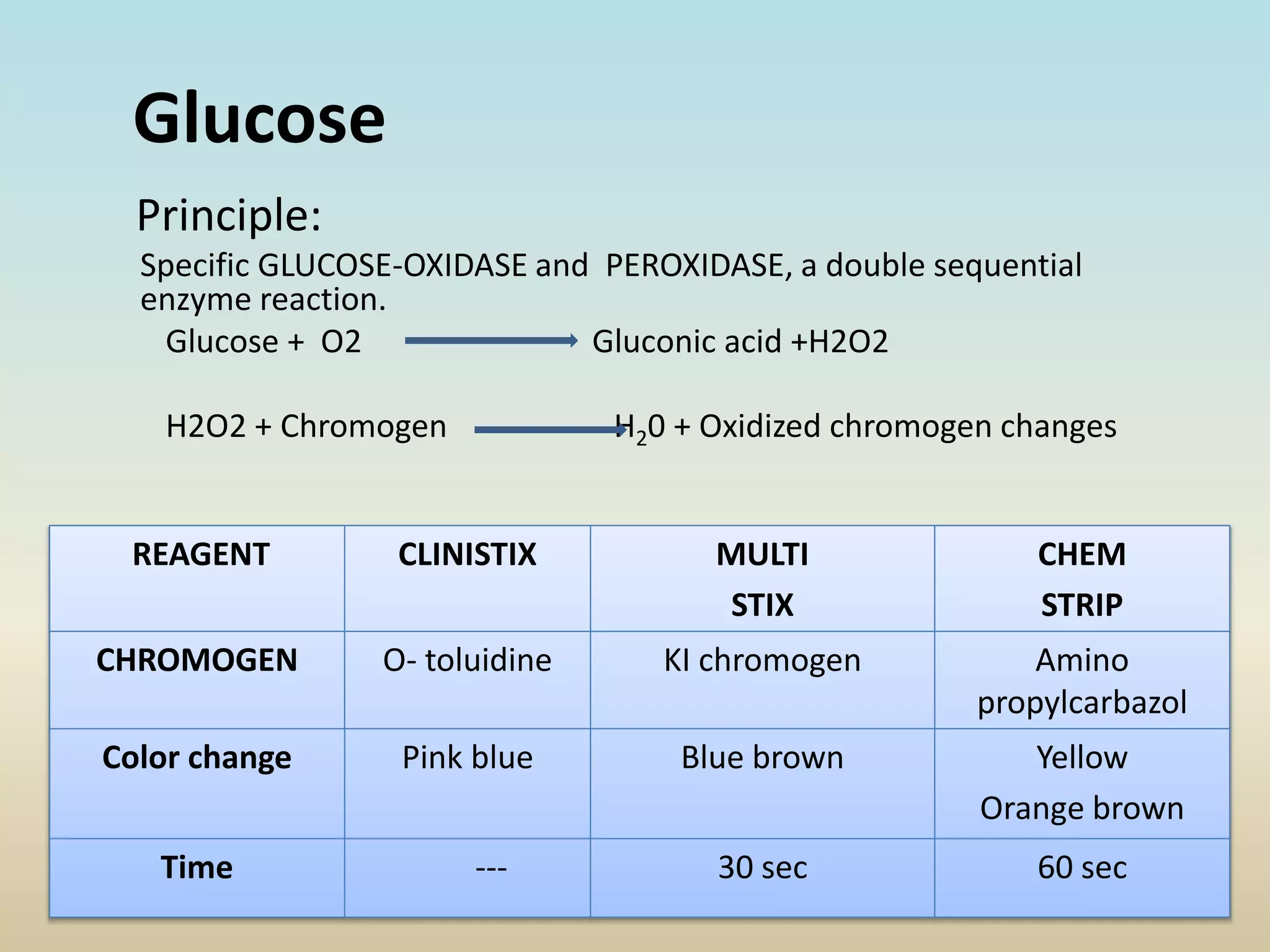
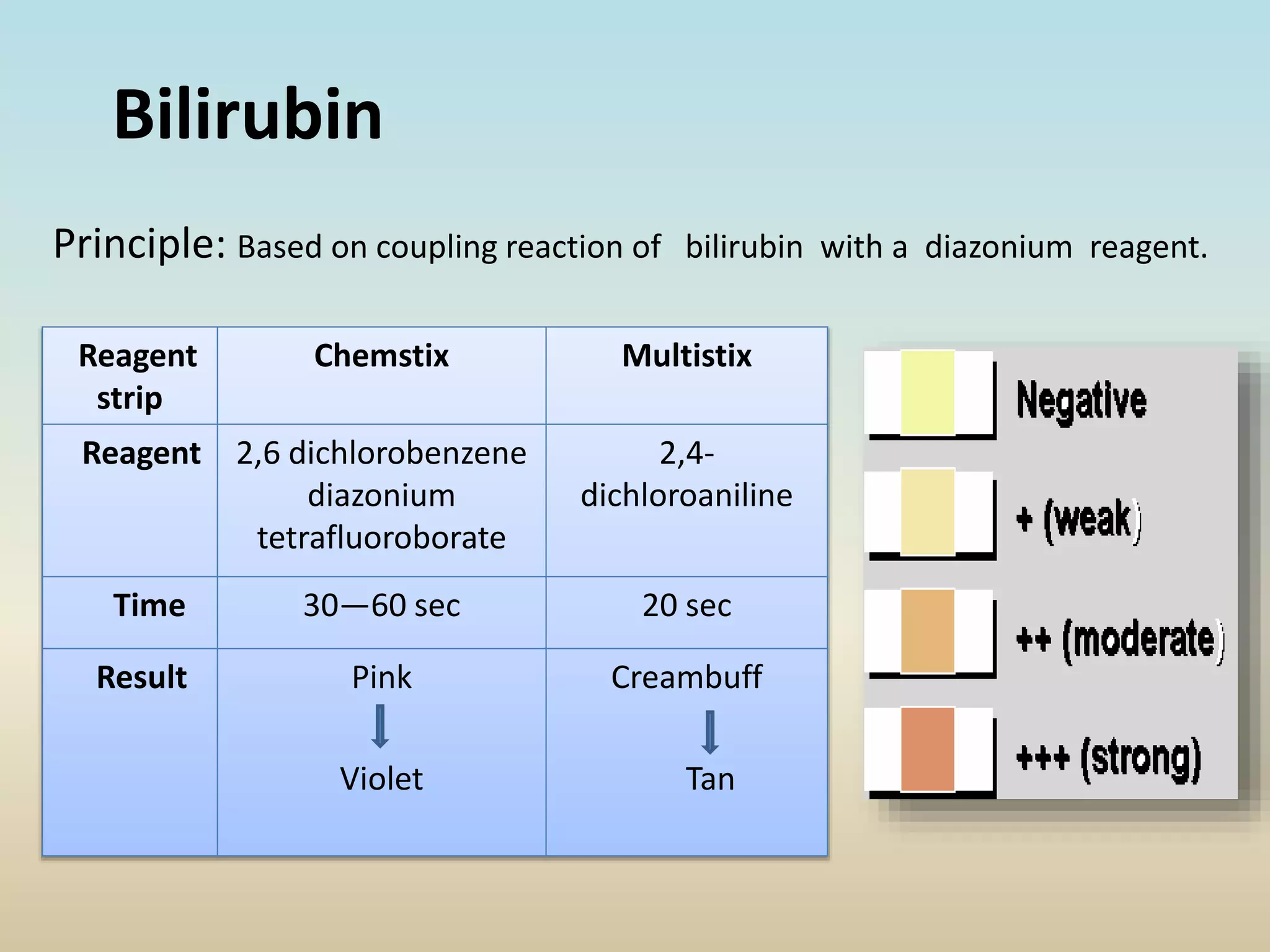
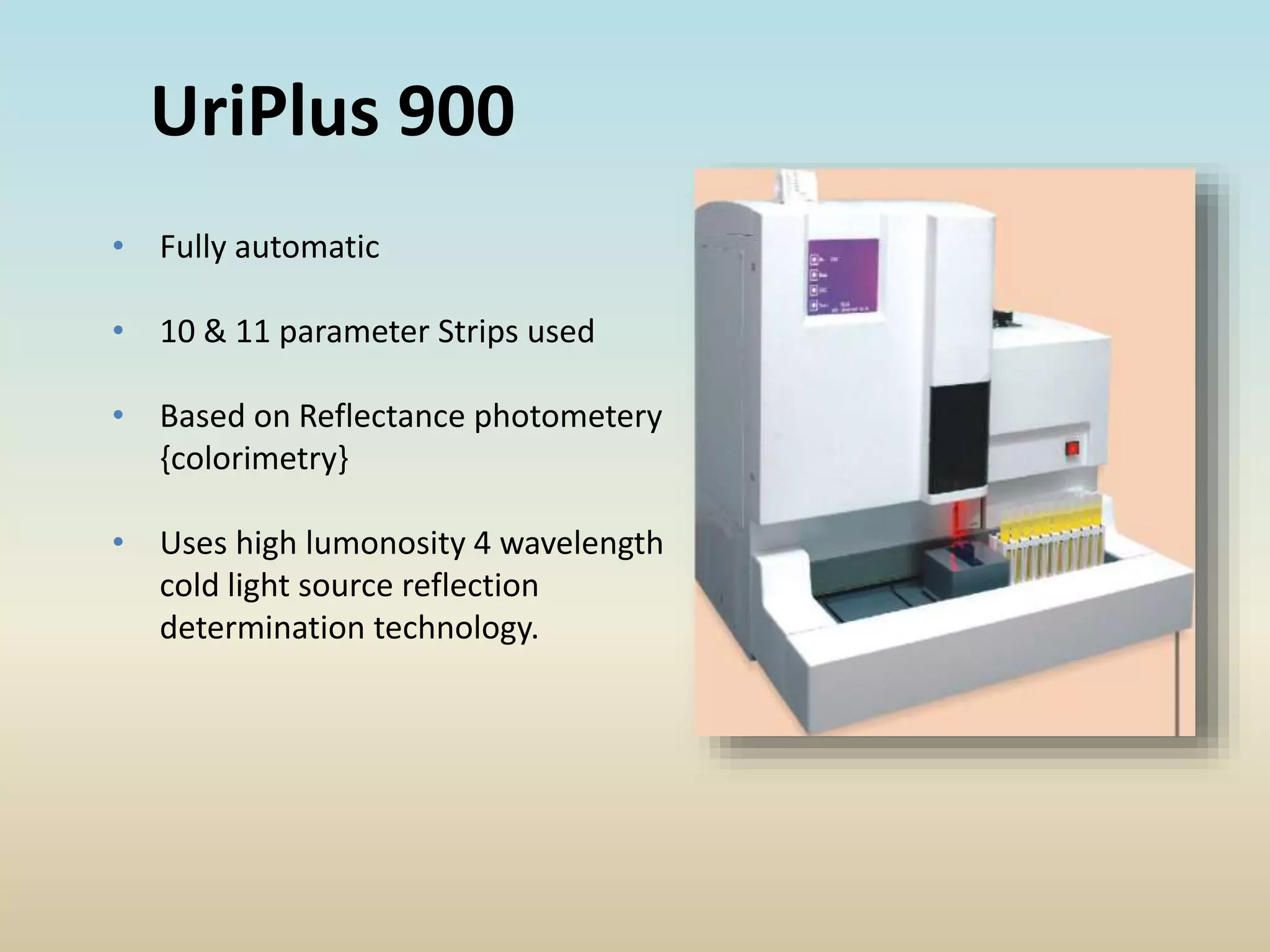
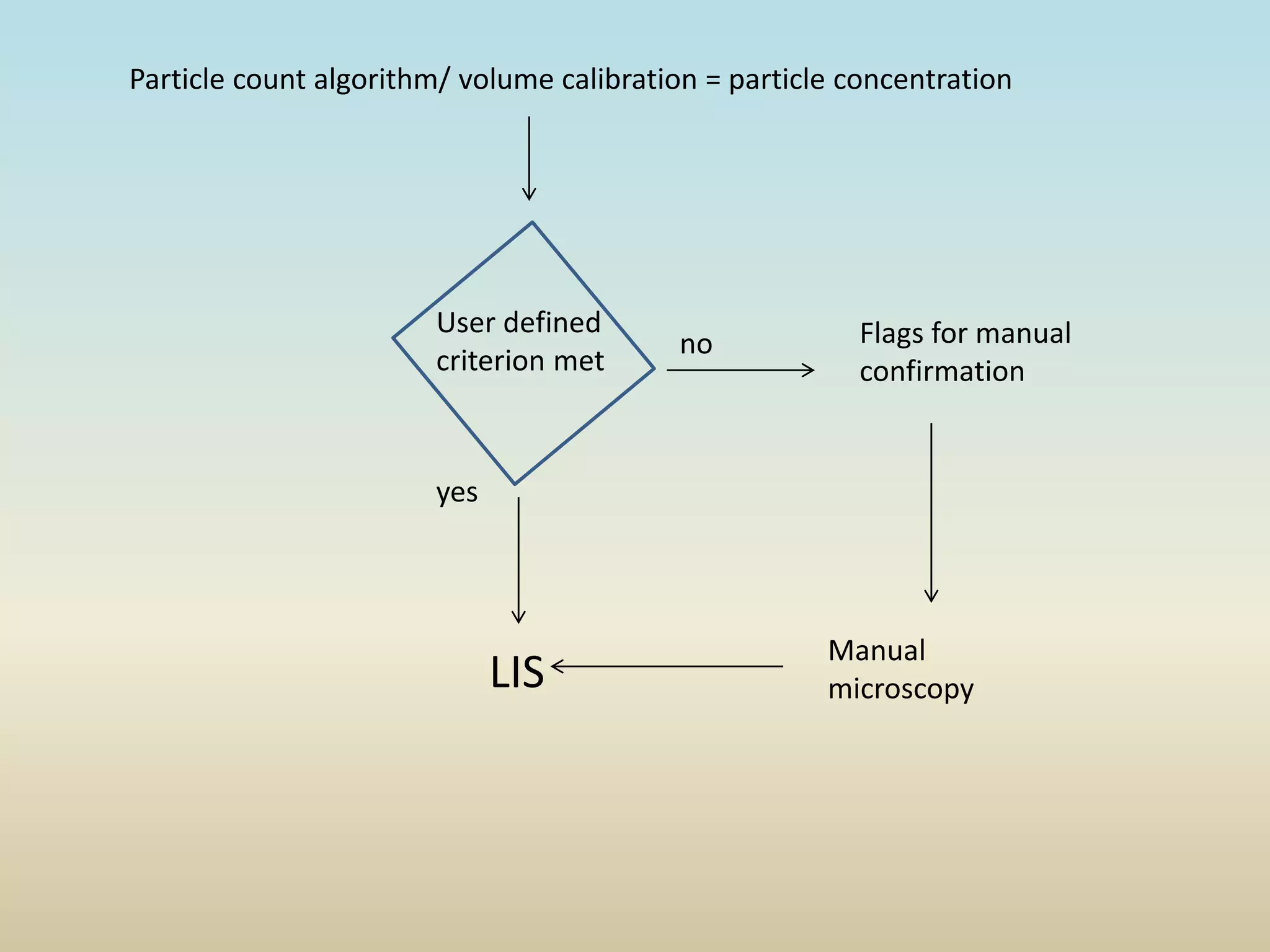
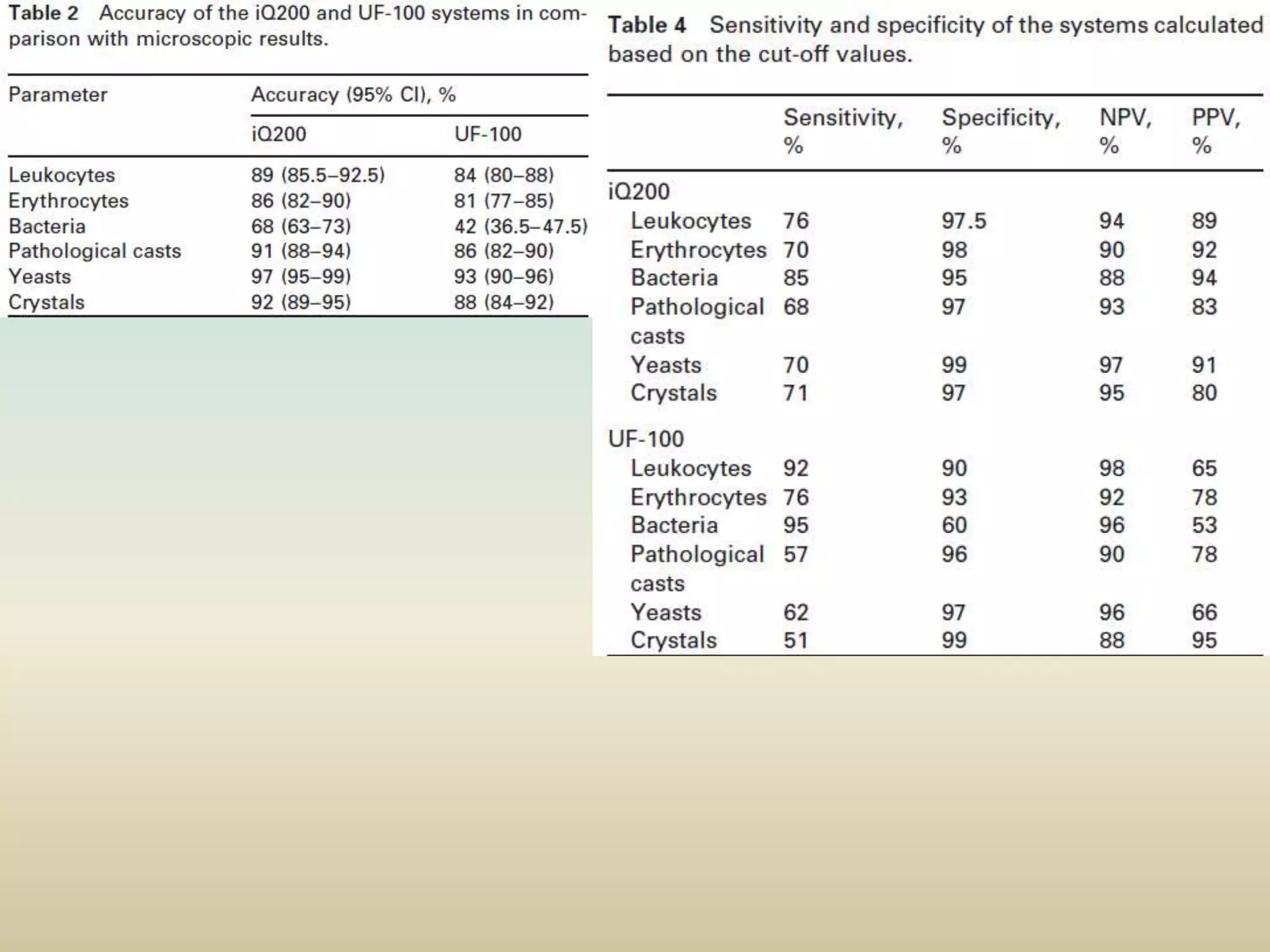
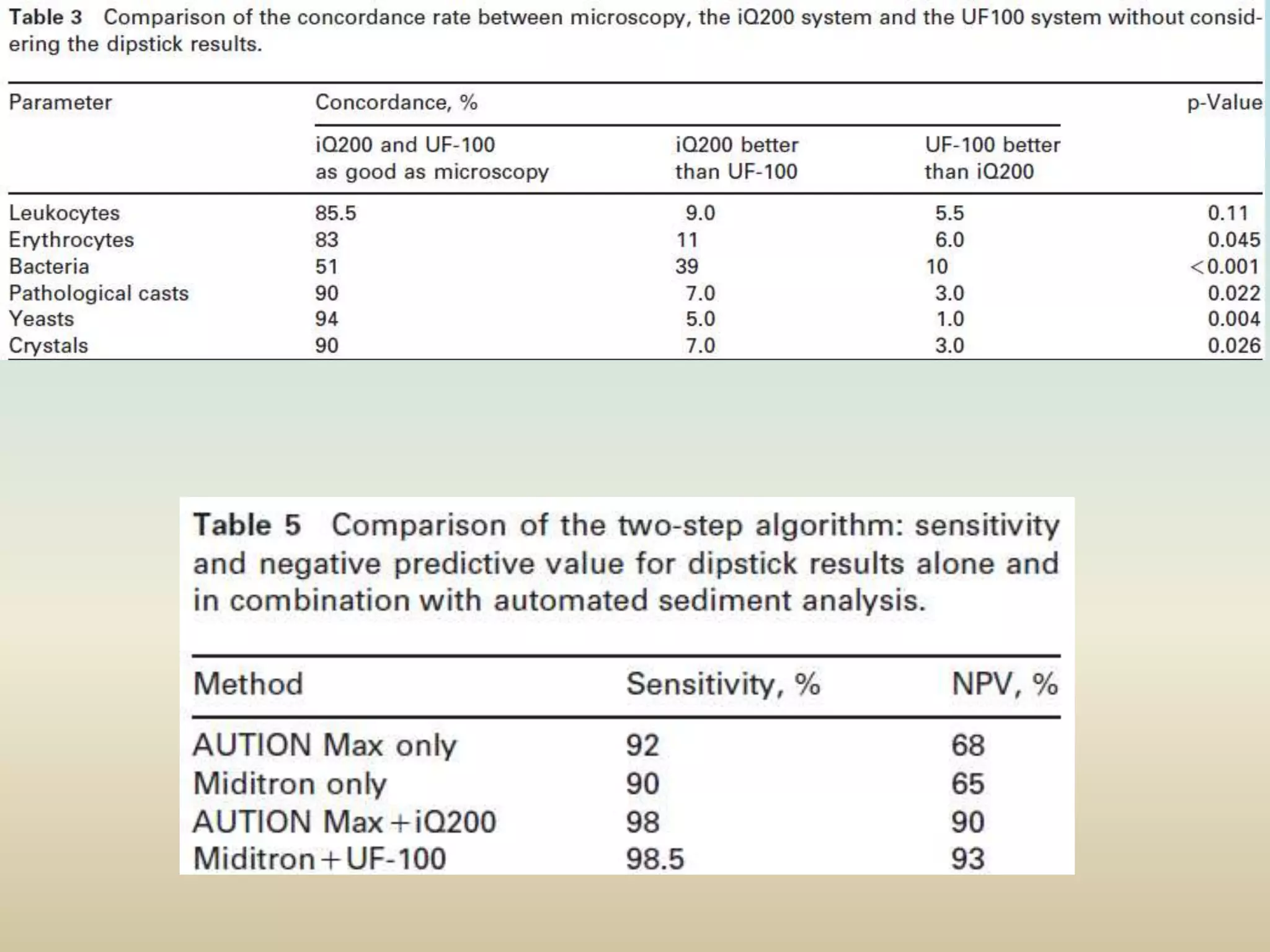
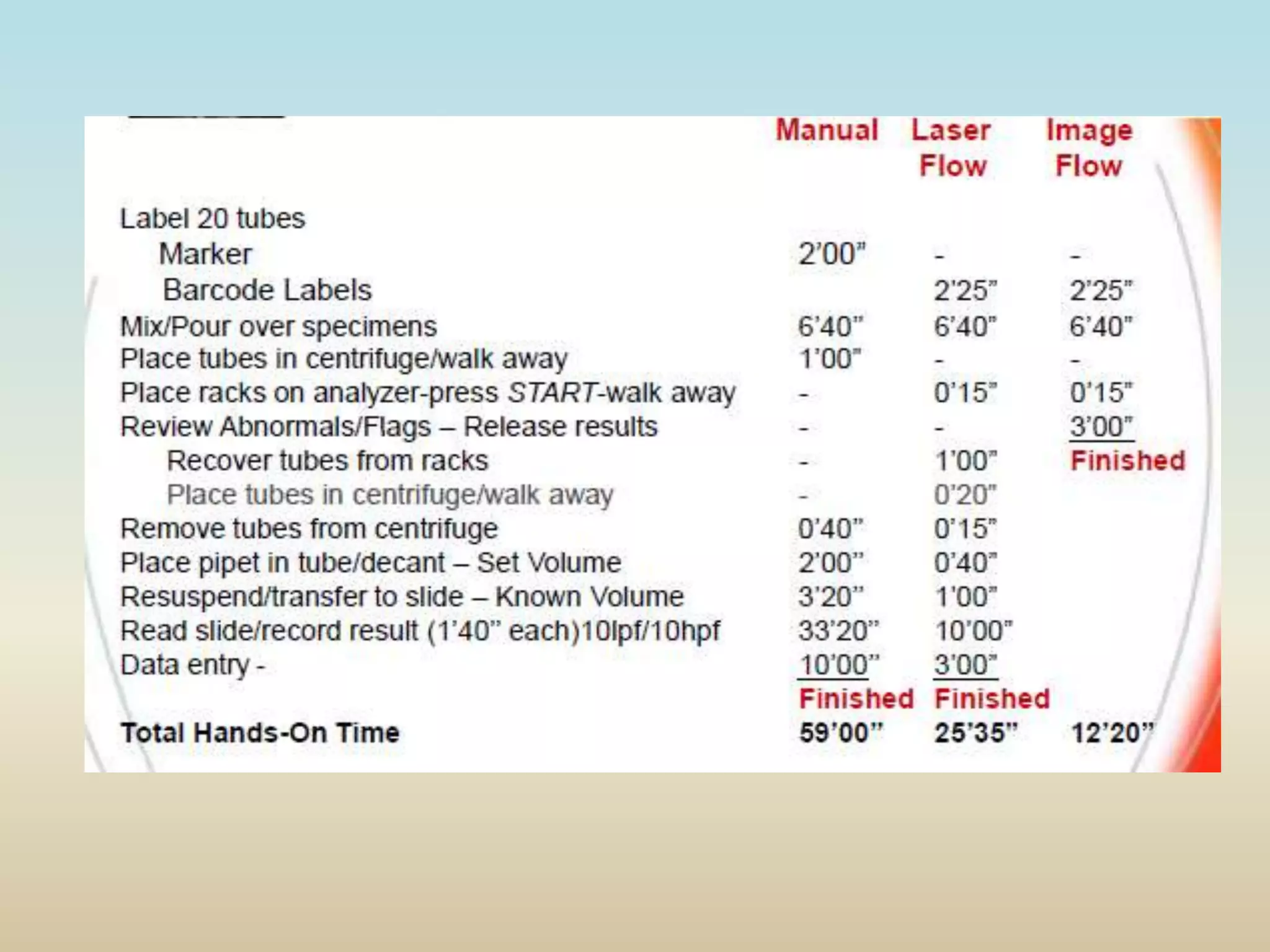
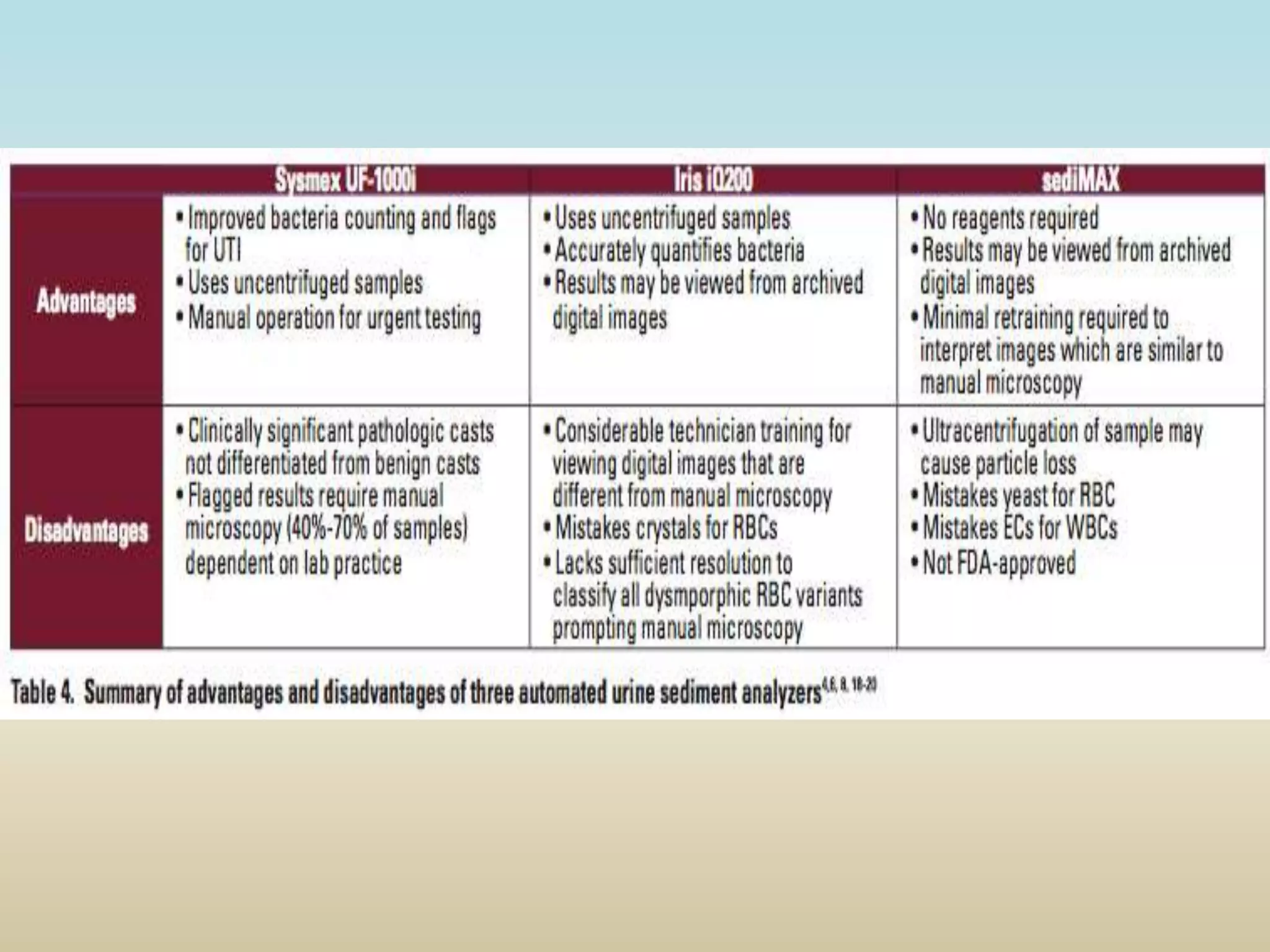
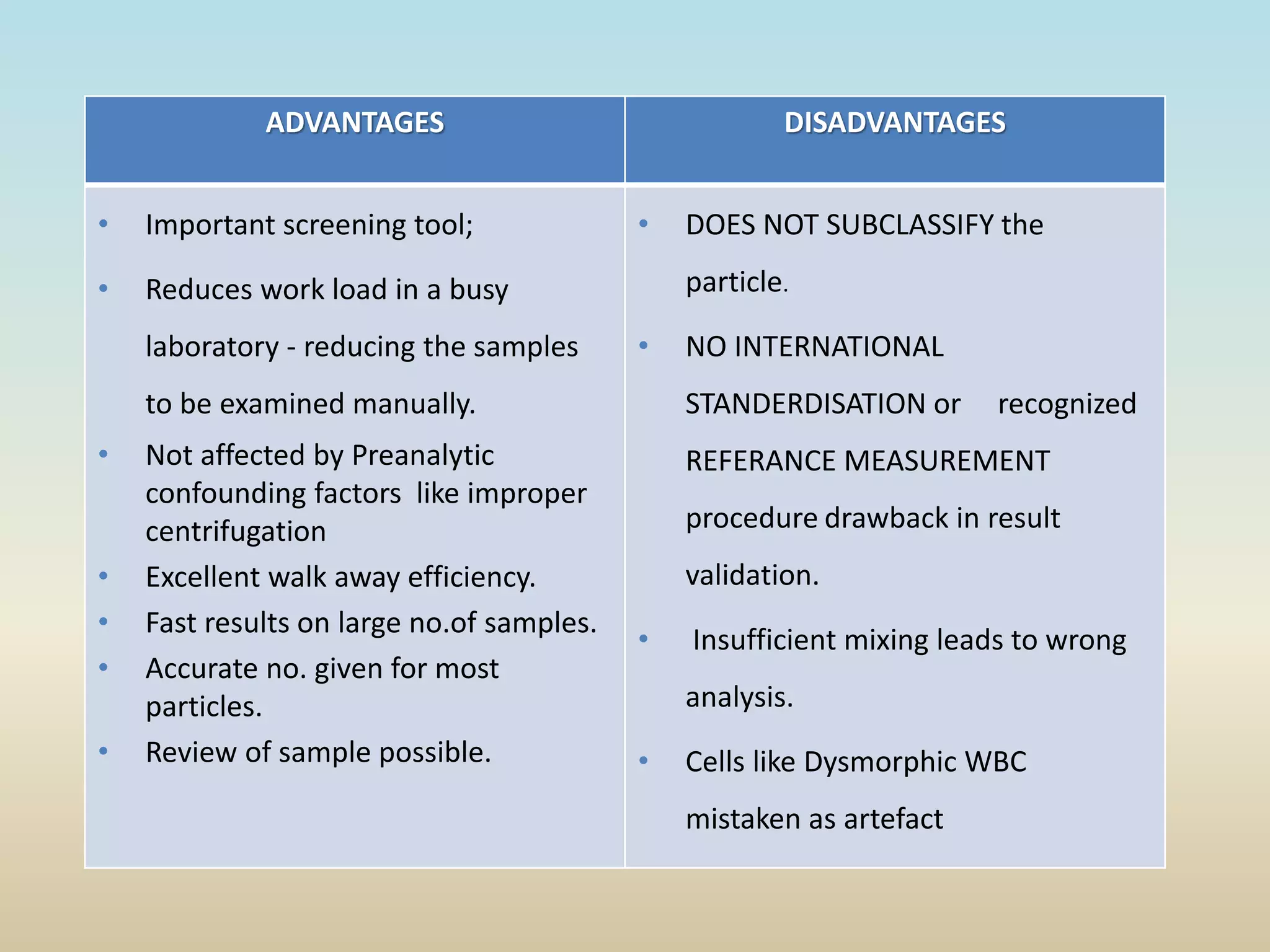
The document discusses the evolution and significance of automation in urine analysis, highlighting the historical use of urine for diagnosing diseases and the technological advancements in testing methods like dipsticks and automated microscopy. It details the processes involved in urine analysis, the benefits of automation such as increased productivity and reduced errors, and emphasizes quality control measures to ensure accurate results. Ultimately, the document underscores the importance of both biochemical and microscopic analyses in pathology identification, advocating for improved laboratory workflows through automation.









































![Clinical microscopy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalmicroscopyautosaved-220927134314-e2d226b7-thumbnail.jpg?width=640&height=640&fit=bounds)




























