Downloaded 555 times


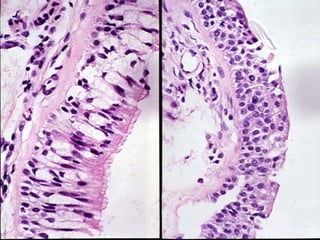
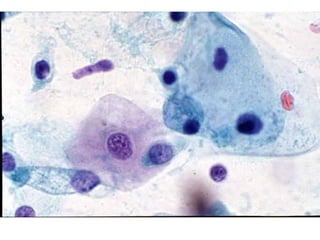
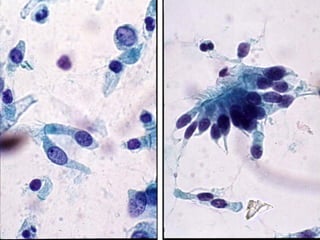
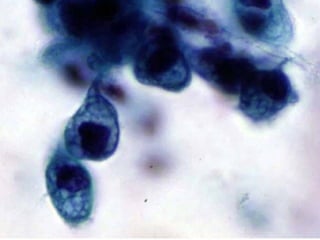

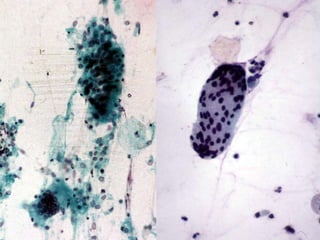
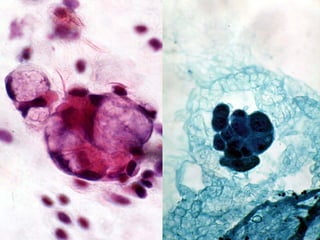
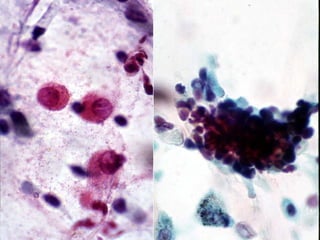
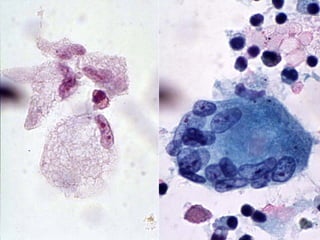

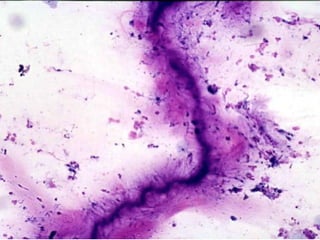

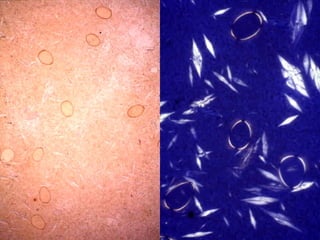
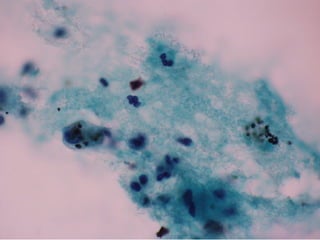

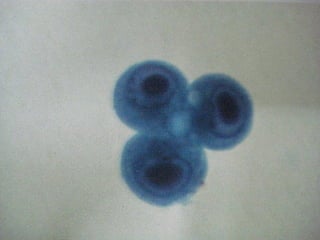
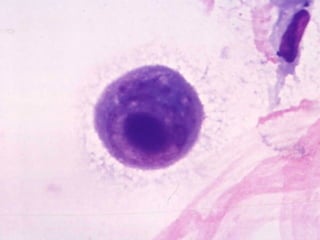
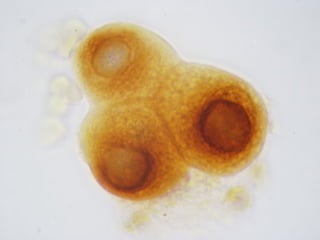
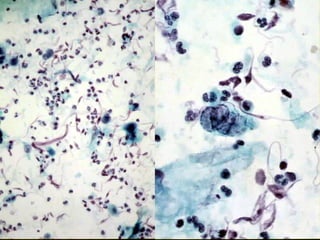

Bronchial cytology and fine needle aspiration are important techniques for diagnosing lung lesions. Bronchial cytology examines the central airways using bronchoscopy while fine needle aspiration can sample peripheral lung lesions. Normal respiratory cells include ciliated bronchial cells and alveolar macrophages. Benign lesions may show goblet cell or basal cell hyperplasia. Non-neoplastic lung diseases like sarcoidosis and pulmonary alveolar proteinosis can also be diagnosed through their characteristic cytology findings. Cytology is useful for identifying infection causes as well as diagnosing and classifying lung tumors.























































































