The document outlines a diagnostic cytopathology session focusing on serous effusions, detailing specimen collection, diagnostic methods, and potential pitfalls in cytopathology. It covers various conditions such as benign and malignant diseases, diagnostic techniques, and case studies to differentiate between them. Emphasis is placed on understanding cytologic features and avoiding misinterpretation in malignant versus benign conditions to improve diagnostic accuracy.
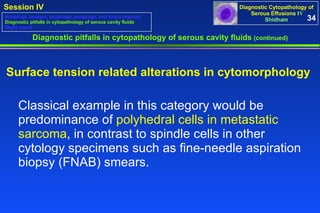
![1 Diagnostic Cytopathology of Serous Effusions Session IV ( 10.50-11.35 ) Q&A- 11.35-12.00 To view this session on web copy-paste the following URL into your browser: http://www.slideshare.net/vshidham/04-presentations-iv-vs-8mb-1042708b-pps Vinod B. Shidham , MD, FRCPath, FIAC Professor Executive editor & coeditor-in-chief, CytoJournal ( www.cytojournal.com ) Department of Pathology Medical College of Wisconsin 9200 W Wisconsin Av, Milwaukee, WI 53226, USA [email_address] 2008 Wisconsin Society of Cytology SPRING MEETING, 40TH ANNIVERSARY Holiday Inn – Riverwalk, Neenah, WI Saturday, April 19, 2008 (7.30 to 3.30)](https://image.slidesharecdn.com/04-presentations-iv-vs-8mb-1042708b-pps-1206654316321-3/85/04-Presentations-IV-VS-8MB-3-28-08-pps-1-320.jpg)

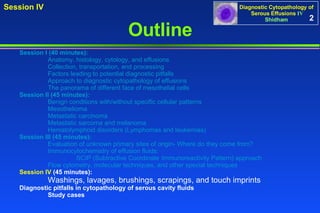

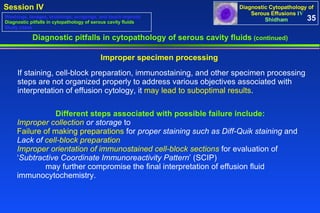
![Metastatic mucinous adenocarcinoma (pleural fluid). Intracytoplasmic mucicarmine positive mucin [Cell block section, Mucicarmine stain] Diagnostic pitfalls in cytopathology of serous cavity fluids (continued) 42 Washings, lavages, brushings, scrapings, and touch imprints Diagnostic pitfalls in cytopathology of serous cavity fluids Study cases](https://image.slidesharecdn.com/04-presentations-iv-vs-8mb-1042708b-pps-1206654316321-3/85/04-Presentations-IV-VS-8MB-3-28-08-pps-43-320.jpg)

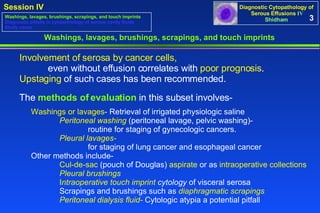
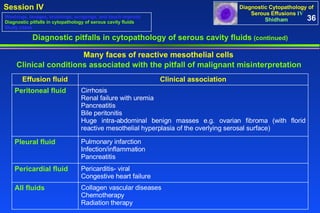
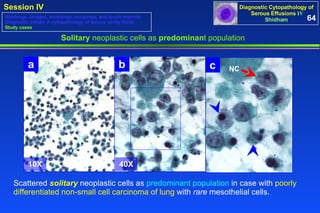
![‘ Subtractive coordinate immunoreactivity pattern’ (SCIP) in cell block sections Metastatic lung carcinoma, (pleural fluid). The specimen show scattered solitary neoplastic cells (red arrows NC) with rare mesothelial cells (blue arrow RM). The neoplastic cells are immunoreactive for pan-cytokeratin (B) and non-immunoreactive for vimentin (A), LCA (C), and calretinin (D). Rare reactive mesothelial cells (blue arrow RM) [with immunoreactivity for calretinin (nuclear-cytoplasmic) (D) and inflammatory cells (arrowhead) [with immunoreactivity for LCA (C)] in the background can be subtracted from neoplastic cells to deduce a diagnostic coordinate immunoreactivity pattern. This is consistent with poorly cohesive singly scattered carcinoma cells, which were also non-immunoreactive for the melanoma marker. Nuclear immunoreactivity for TTF-1 (E) with a clinical history of lung mass is consistent with a lung primary. 63 HE stained cell block section 40X 100X D. Calretinin Non-immunoreactive (Mesothelial cell- immunoreactive nuclear-cytoplasmic) E. TTF-1 Immunoreactive nuclear 40X 100X B. Pan-cytokeratin Immunoreactive C. LCA (CD45) Non-immunoreactive 40X 40X 100X 100X 40X 100X A. Vimentin Non-immunoreactive NC RM NC RM NC](https://image.slidesharecdn.com/04-presentations-iv-vs-8mb-1042708b-pps-1206654316321-3/85/04-Presentations-IV-VS-8MB-3-28-08-pps-64-320.jpg)
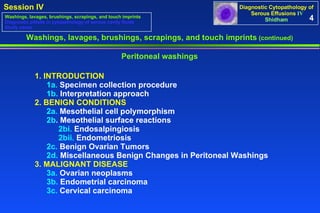
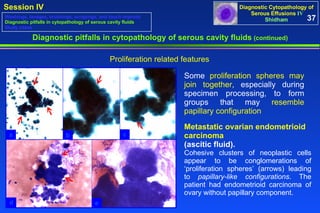
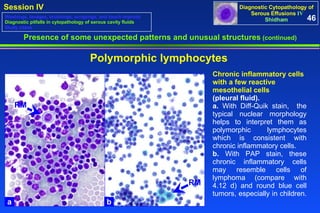
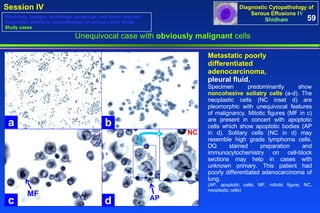
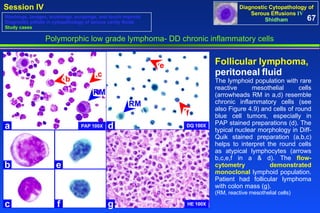
![Large B-cell lymphoma , peritoneal fluid. PAP stained Cytospin preparations (a through c) showed non-cohesive solitary cells (red arrow NC in c) with many apoptotic bodies (arrowheads in c). These cells in PAP stained preparations resemble non-cohesive poorly differentiated non-small cell carcinoma with a solitary cell pattern. They are present in the HE stained cell-block section as small groups (d). By the SCIP approach neoplastic cells could be separated out from cytokeratin 7 (A) and calretinin (B) immunoreactive mesothelial cells (blue arrow RM). After following them in serial sections, the neoplastic cells (red arrow NC) were immunoreactive for CD20 (C) and non-immunoreactive for CD3 (E). They expressed Bcl2 (D). Flow cytometry demonstrated the monoclonal nature of the CD20 immunoreactive cells. The patient had lymphoma of the small bowel. This was a consult case and a DQ stained preparation, which usually is helpful to evaluate lymphoma cells, was not available. (NC, neoplastic cell; RM, reactive mesothelial cell) ‘ Subtractive coordinate immunoreactivity Pattern’ (SCIP) in cell block sections 65 HE stained cell block Section (d) A. Cytokeratin 7 Non-immunoreactive [Mesothelial cell Immunoreactive (red arrow) Cytoplasmic] B. Calretinin Non-immunoreactive [Mesothelial cell Immunoreactive (red arrow) nuclear-cytoplasmic] D. Bcl2 Immunoreactive Cytoplasmic (red arrow) E. CD3 Non-immunoreactive C. CD 20 Immunoreactive Cytoplasmic (red arrow) PAP stained Cytospin preparation (a-c) 40X 40X 40X 40X 40X a b c d 10X 40X NC NC RM NC RM NC NC 40X](https://image.slidesharecdn.com/04-presentations-iv-vs-8mb-1042708b-pps-1206654316321-3/85/04-Presentations-IV-VS-8MB-3-28-08-pps-66-320.jpg)
![Thank you Milwaukee Art Museum [email_address] End Diagnostic Cytopathology of Serous Effusions IV](https://image.slidesharecdn.com/04-presentations-iv-vs-8mb-1042708b-pps-1206654316321-3/85/04-Presentations-IV-VS-8MB-3-28-08-pps-70-320.jpg)