Downloaded 197 times



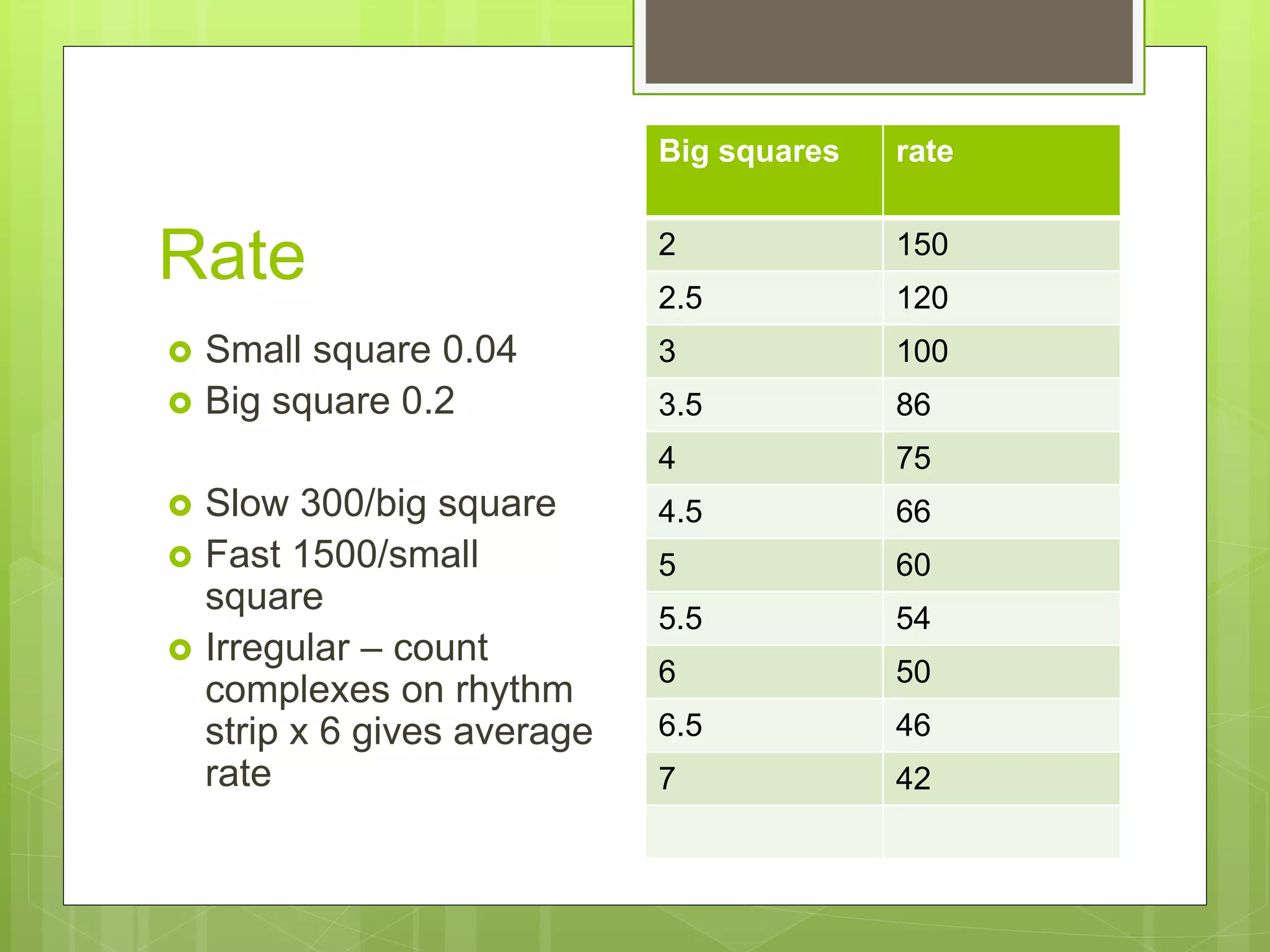
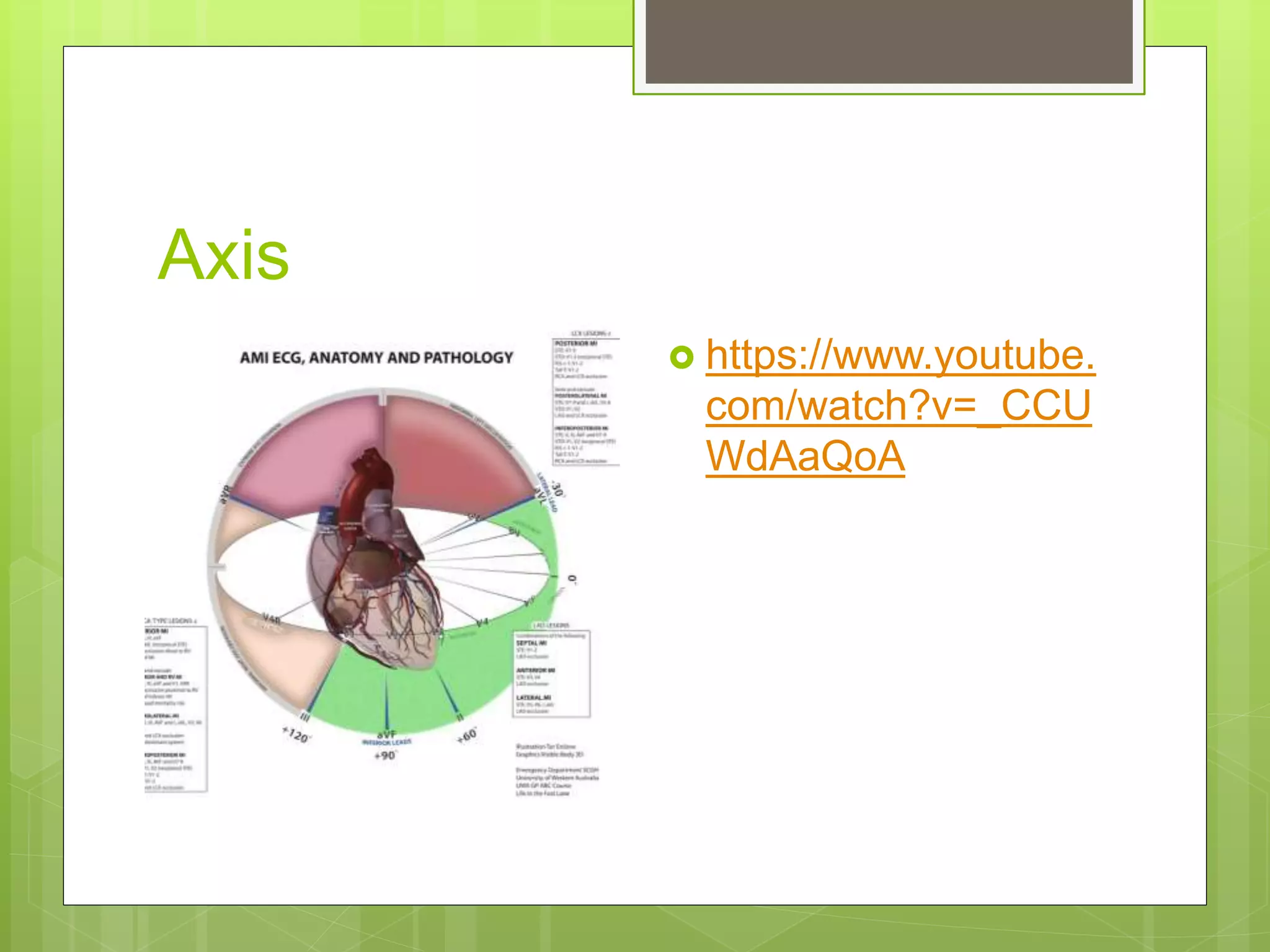


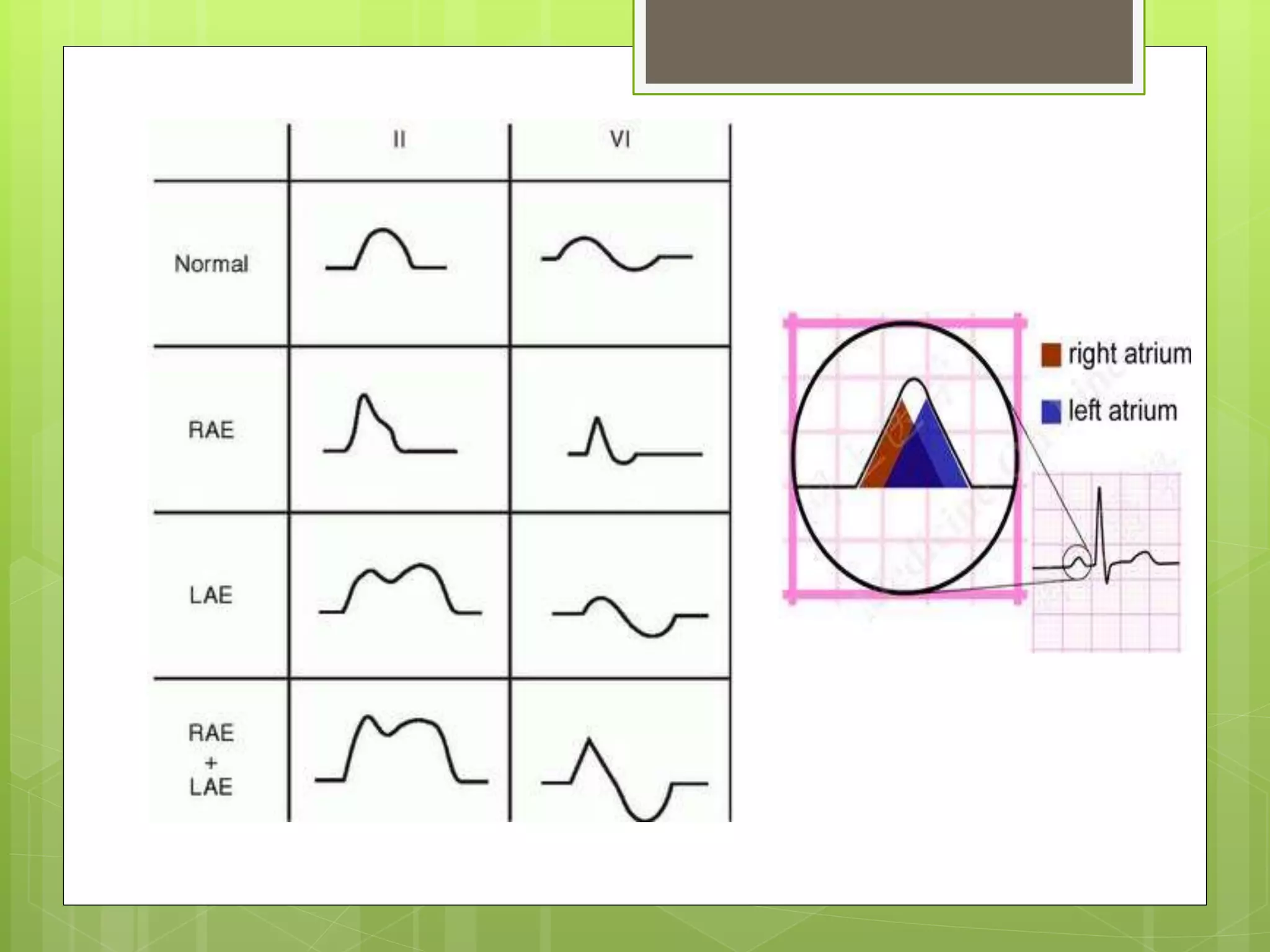
















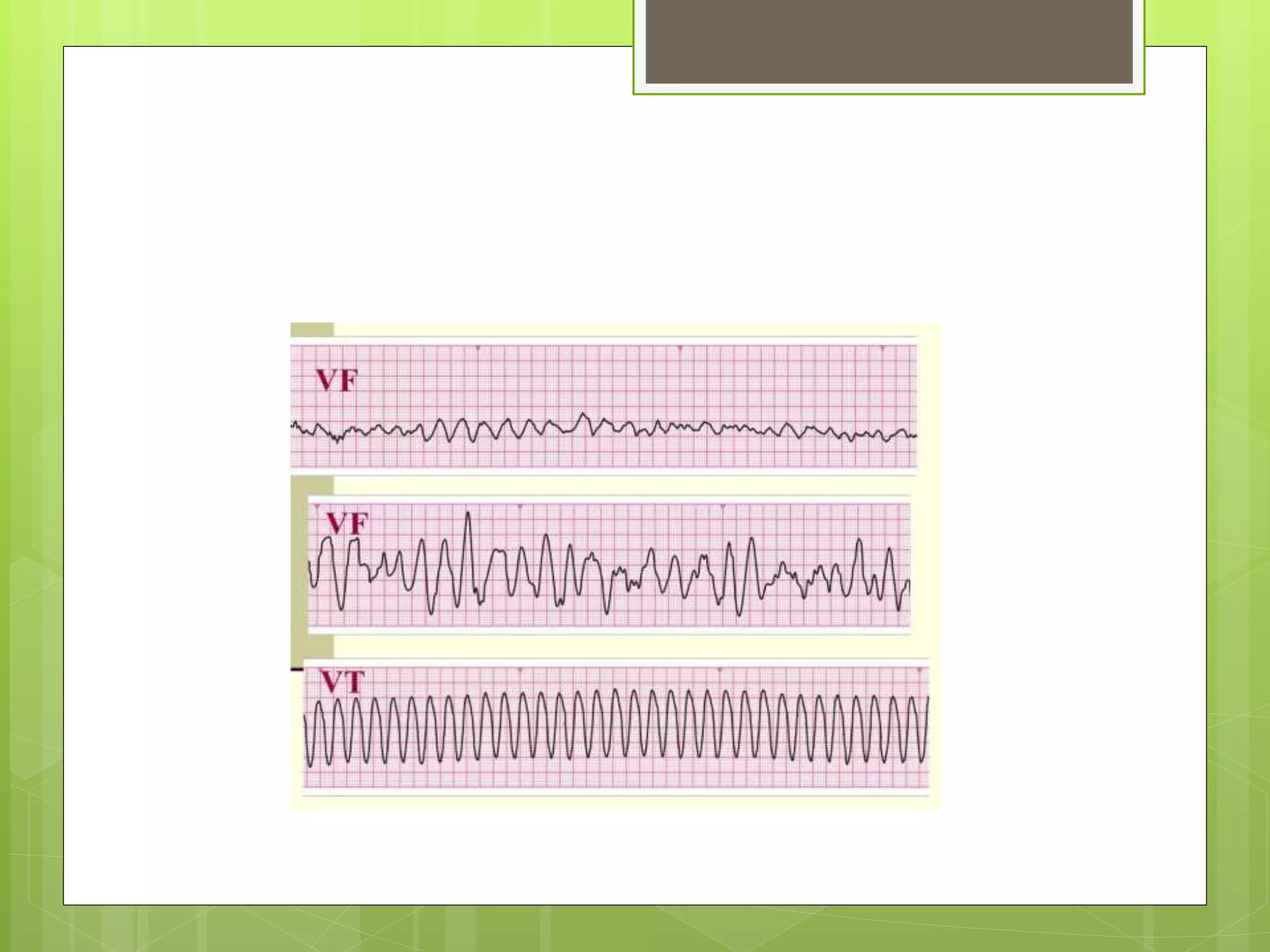

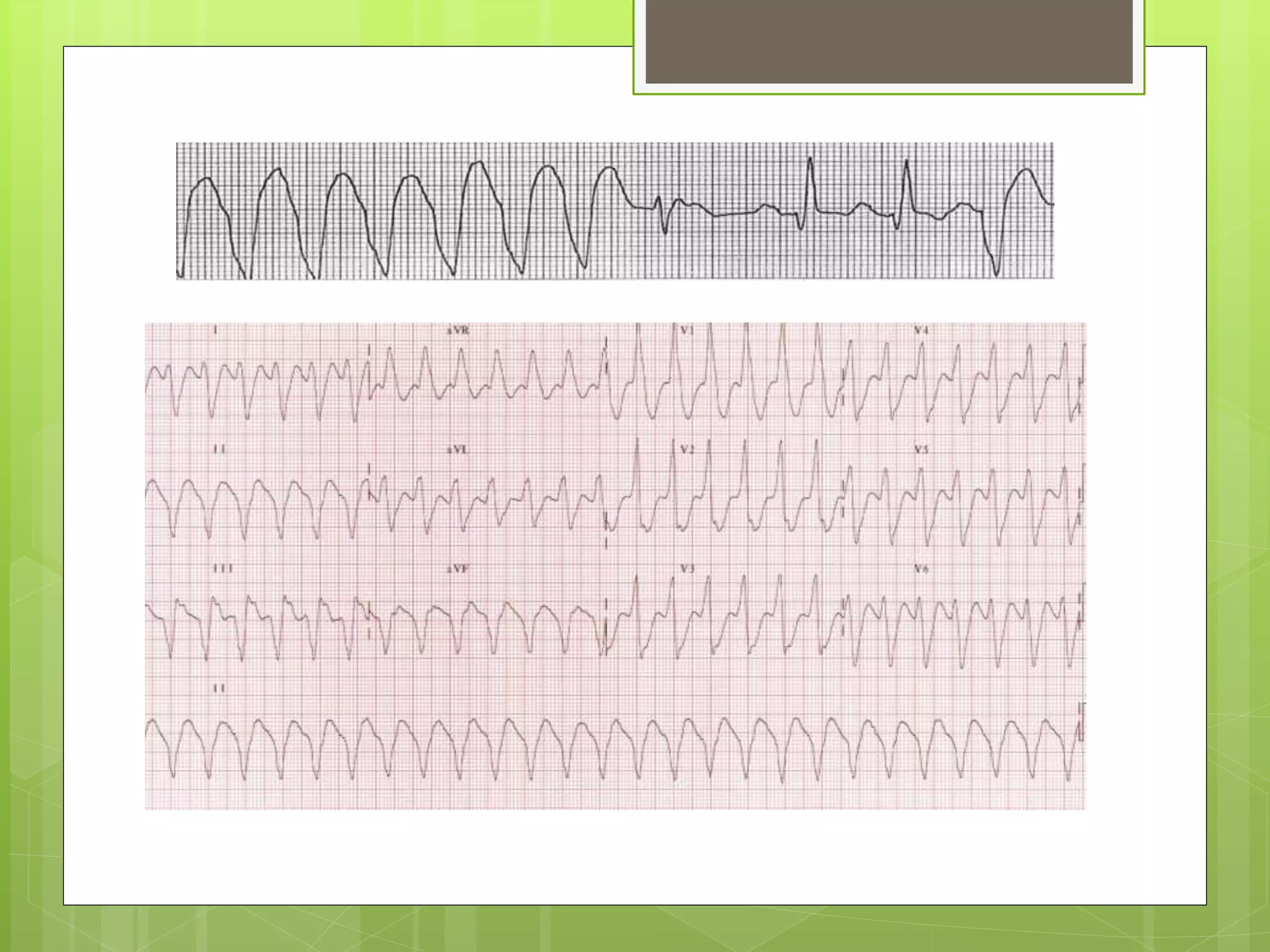

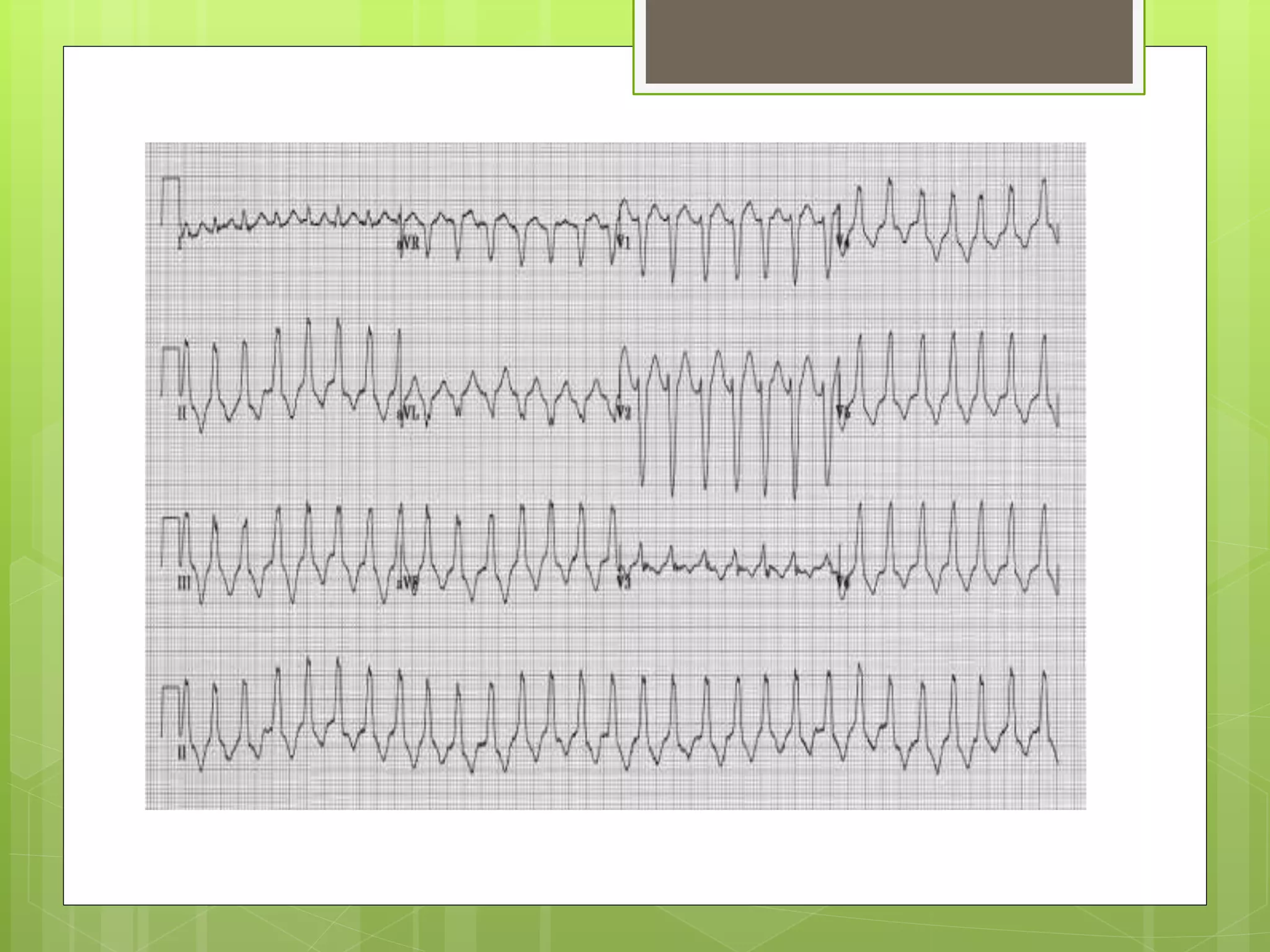

This document provides an overview of systematic ECG interpretation. It discusses the key components that should be analyzed in an ECG including rate, rhythm, axis, P wave, PR interval, QRS complex, QT interval, ST segment, and other waves. For each component, the document outlines what should be assessed such as amplitude, duration, and abnormalities. It also reviews conditions that can cause abnormalities in various ECG components, such as left ventricular hypertrophy, right ventricular hypertrophy, bundle branch blocks, and long QT syndrome. The document emphasizes a systematic approach to ECG interpretation and provides guidance on evaluating rhythms, pediatric considerations, and differentiating ventricular arrhythmias from supraventricular arrhythmias with aberran

































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








