This document provides an overview of electrocardiography (ECG) basics including:
1. It describes what an ECG is and what conditions it can be useful for diagnosing.
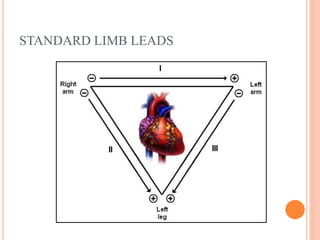
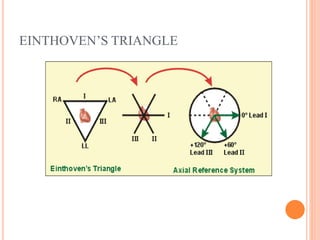
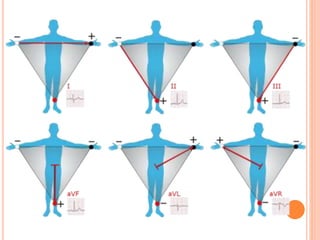
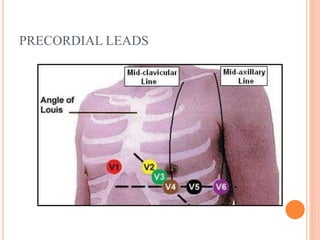
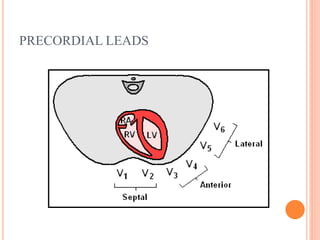
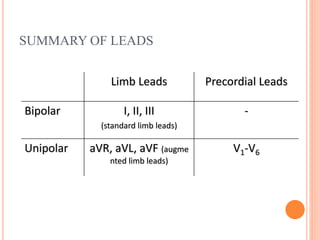
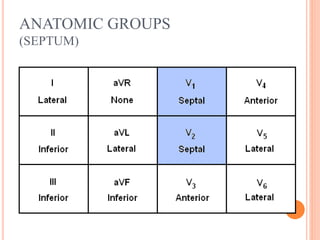
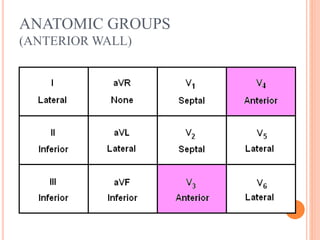
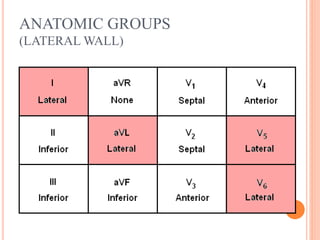
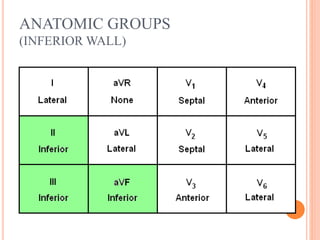
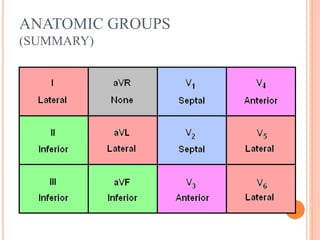
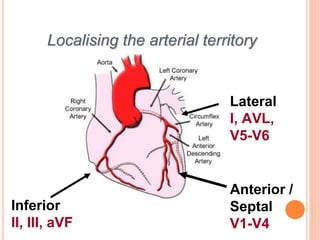
2. It outlines the different ECG leads including the standard and precordial leads used to measure electrical activity from different angles.
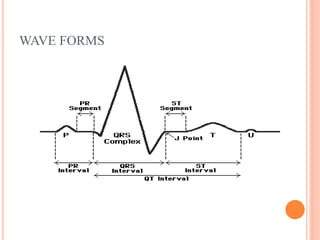
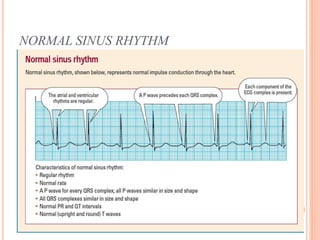
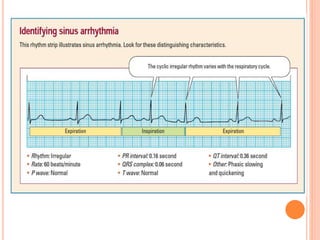
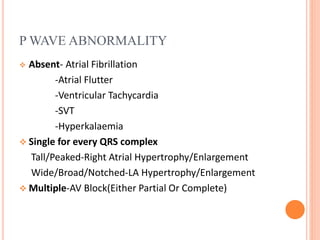
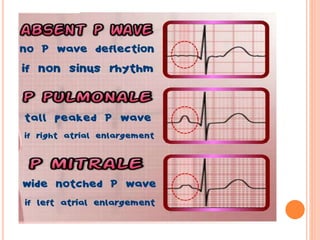
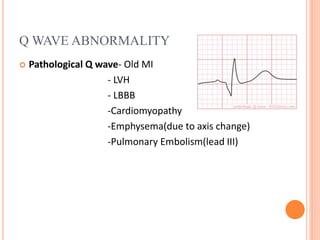
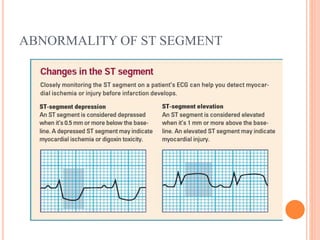
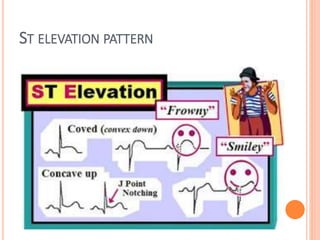
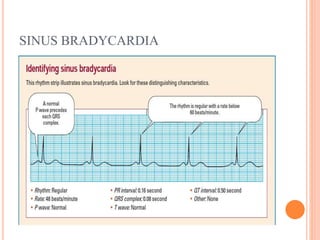
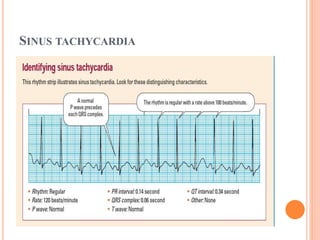
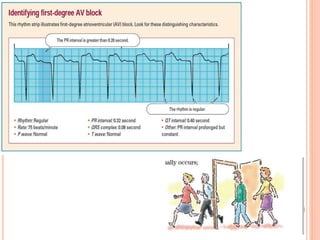
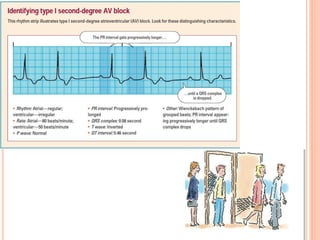
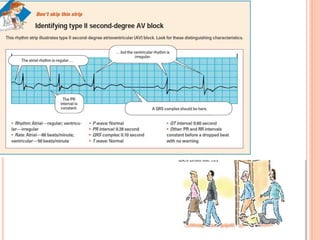
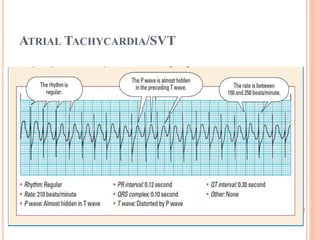
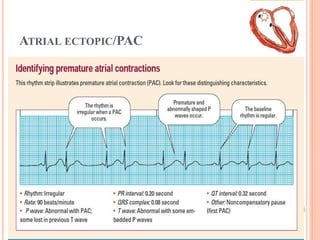
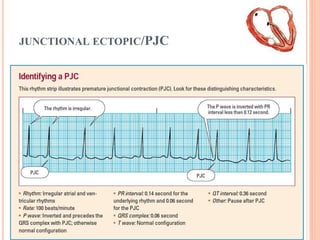
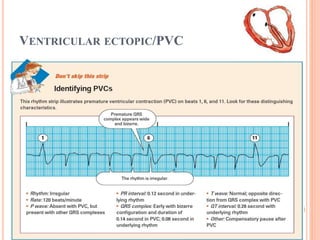
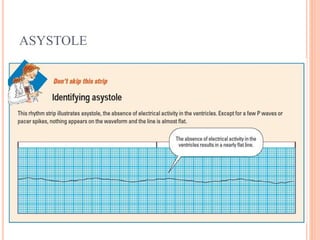
3. It explains the typical ECG waveforms including the P, QRS, T, and U waves as well as intervals like the PR and QT, and how to interpret abnormalities.
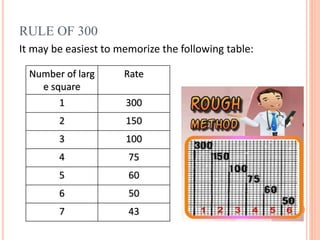
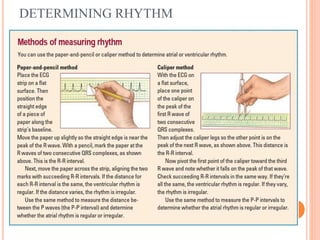
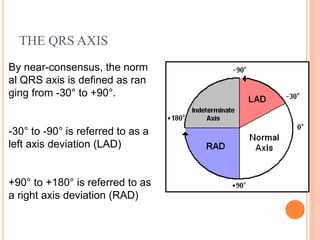
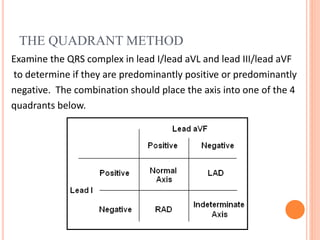
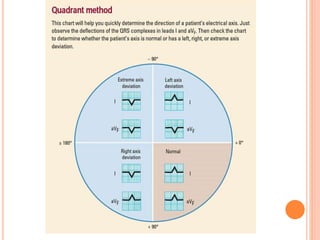
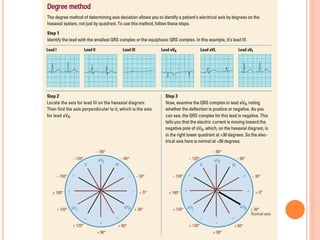
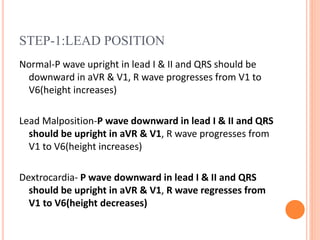
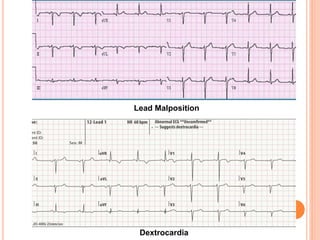
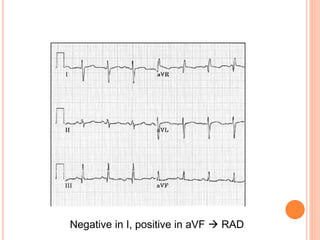
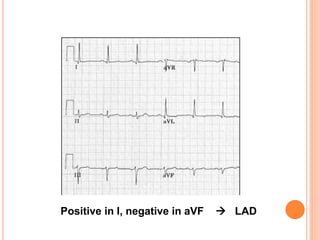
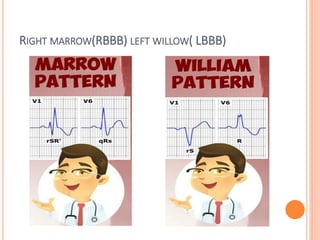
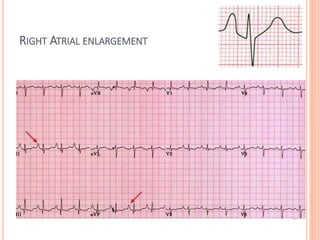
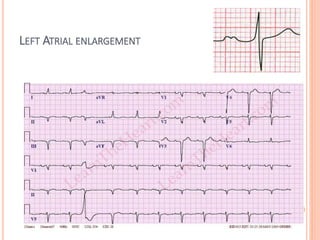
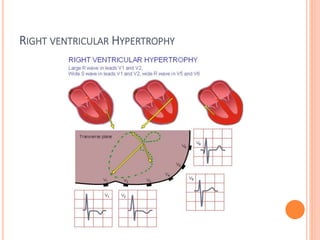
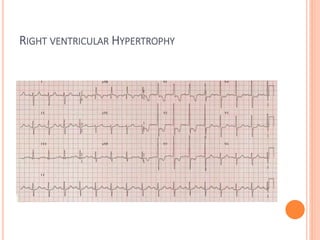
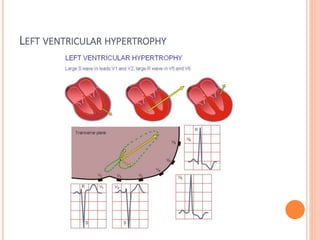
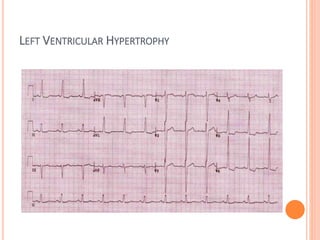
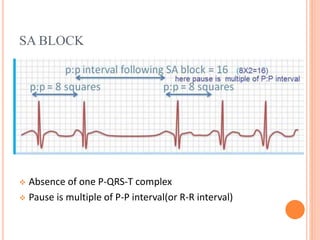
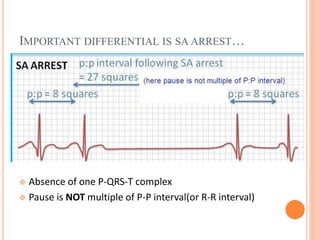
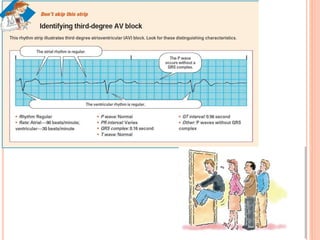
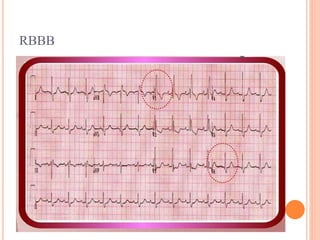
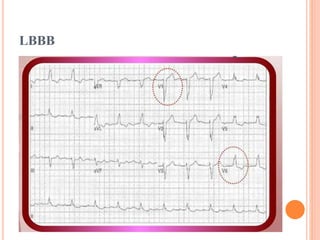
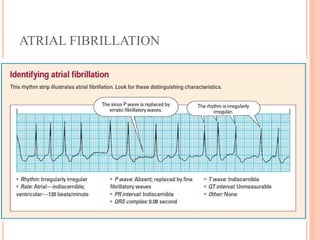
4. It provides guidance on interpreting an ECG including assessing lead position, rhythm, rate, axis, and looking for signs of conditions like bundle branch blocks or chamber enlargement.