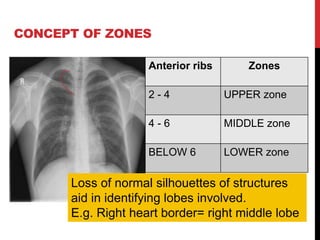
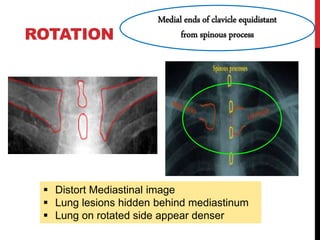
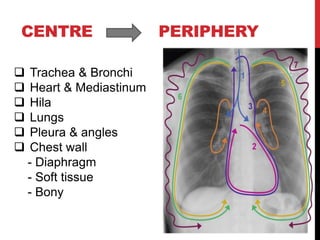
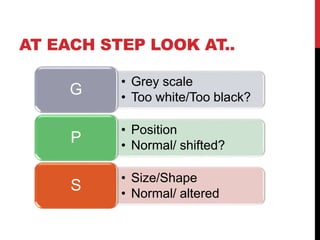
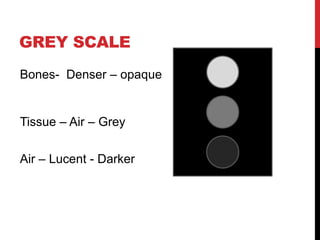
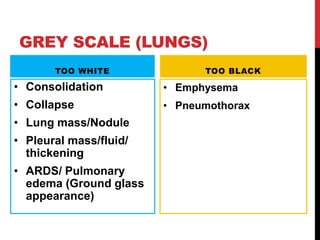
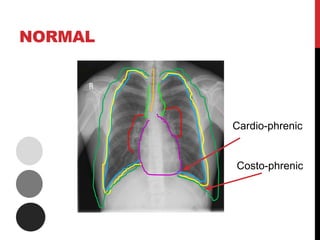
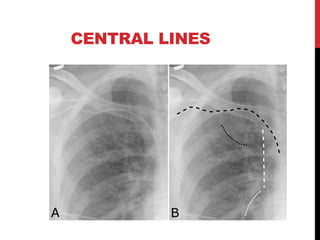
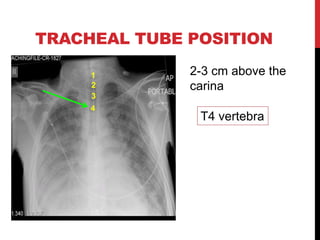
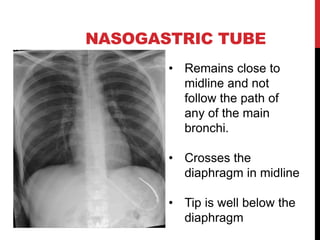
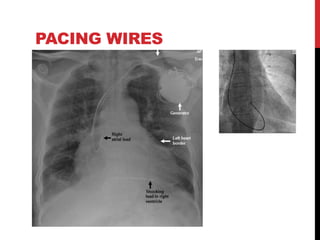
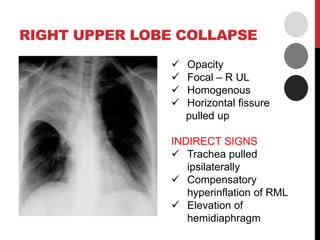
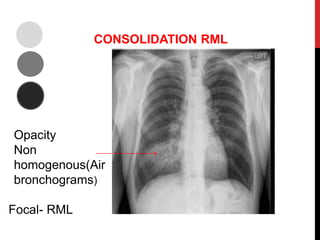
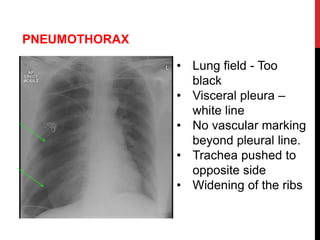
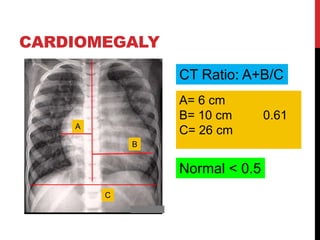
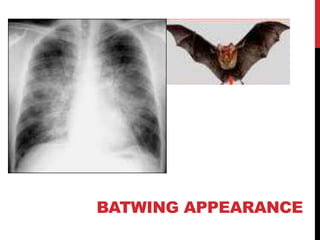
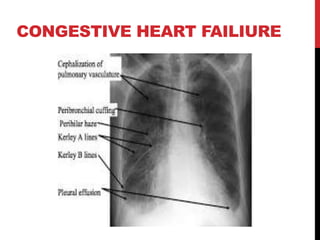
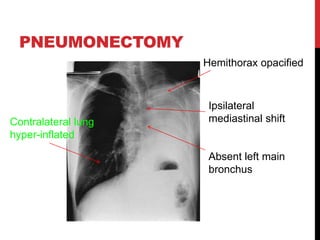
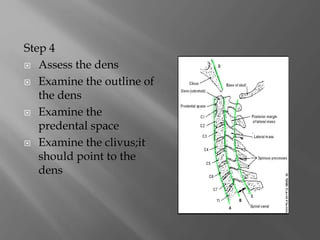
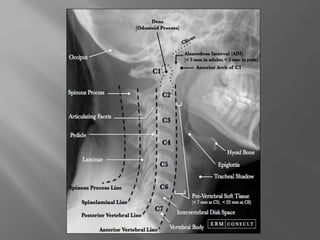
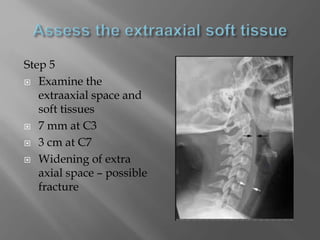
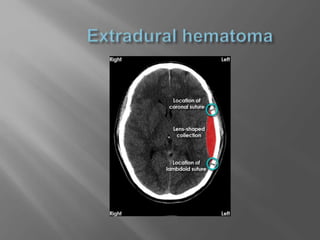
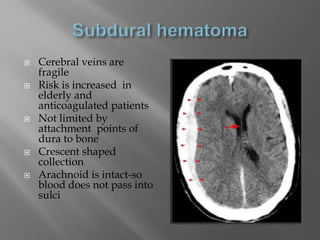
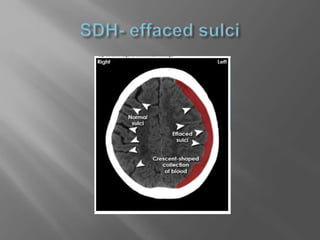
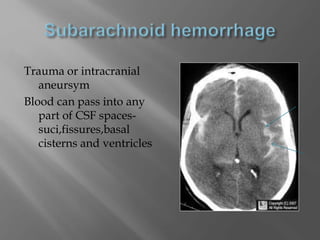
This document provides guidance on reading and interpreting chest x-rays. It begins by identifying the different lung zones and providing a stepwise approach to examining a CXR, including assessing technical quality, position, inspiration, exposure, and rotation. It then describes how to systematically examine the image from center to periphery, looking at grey scale, position, size and shape of structures at each step. Common findings are described, such as consolidation, pneumothorax, cardiomegaly, and foreign bodies. Guidance is also provided on interpreting cervical spine x-rays and CT brain images in trauma.