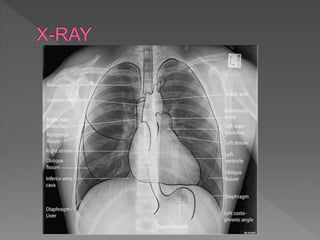
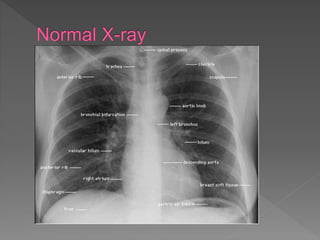
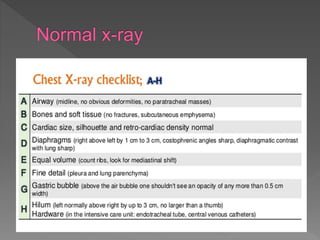
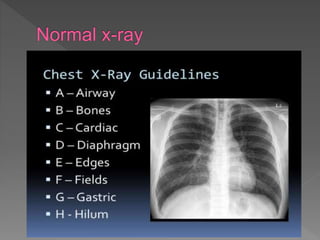
A chest X-ray is used to examine the lungs, heart, bones and soft tissues of the chest. It involves positioning the body between an X-ray machine and plate. Different tissues absorb X-rays at different levels, appearing white, grey or black, allowing visualization of internal structures. A chest X-ray technician must carefully position the patient and ensure proper inspiration and penetration in order to obtain a high quality image for diagnostic purposes. Key areas that are examined include the heart, lungs, bones, diaphragm and chest wall. Abnormalities may be detected by assessing size, shape, positioning and visibility of anatomical structures.