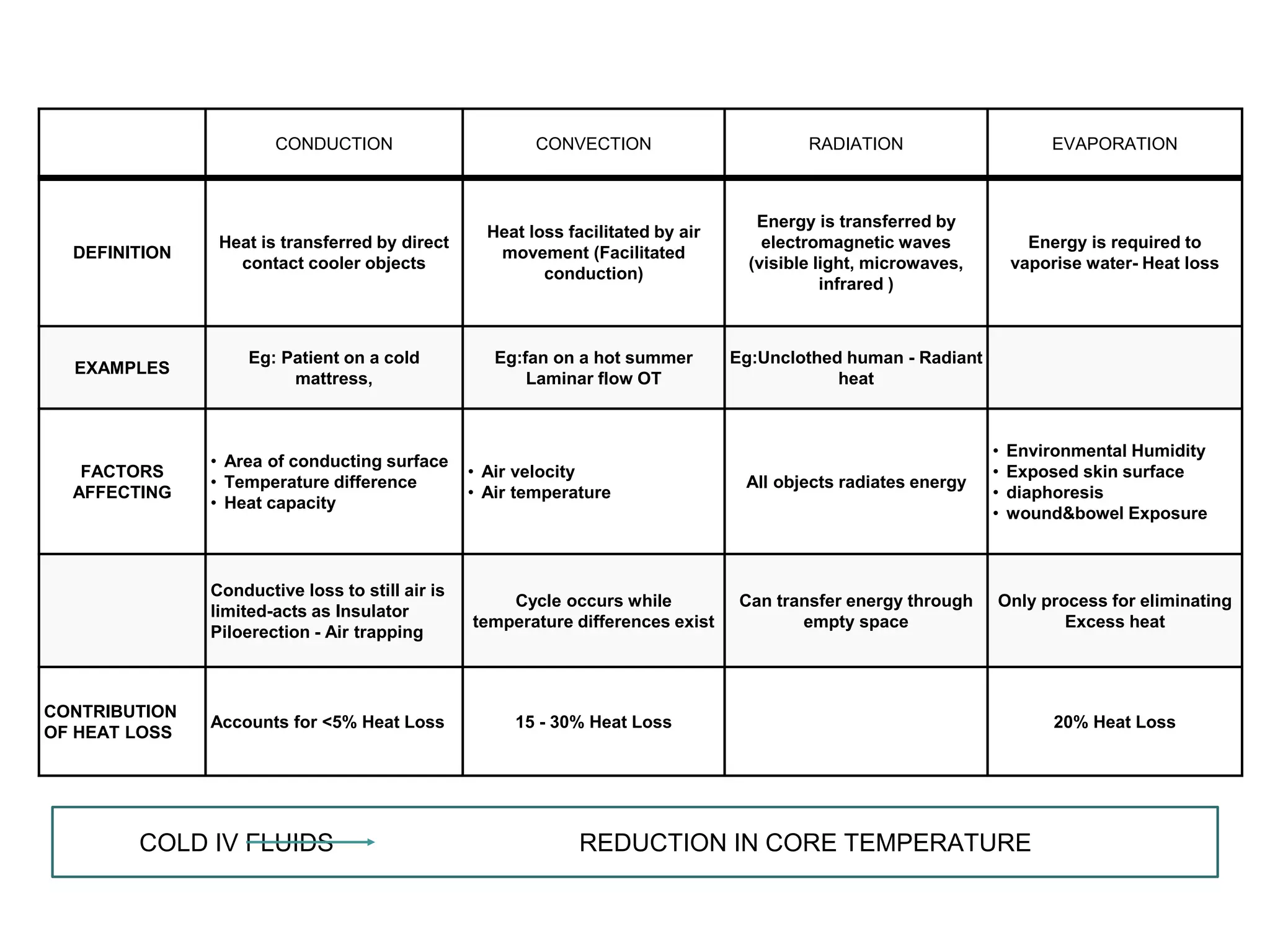
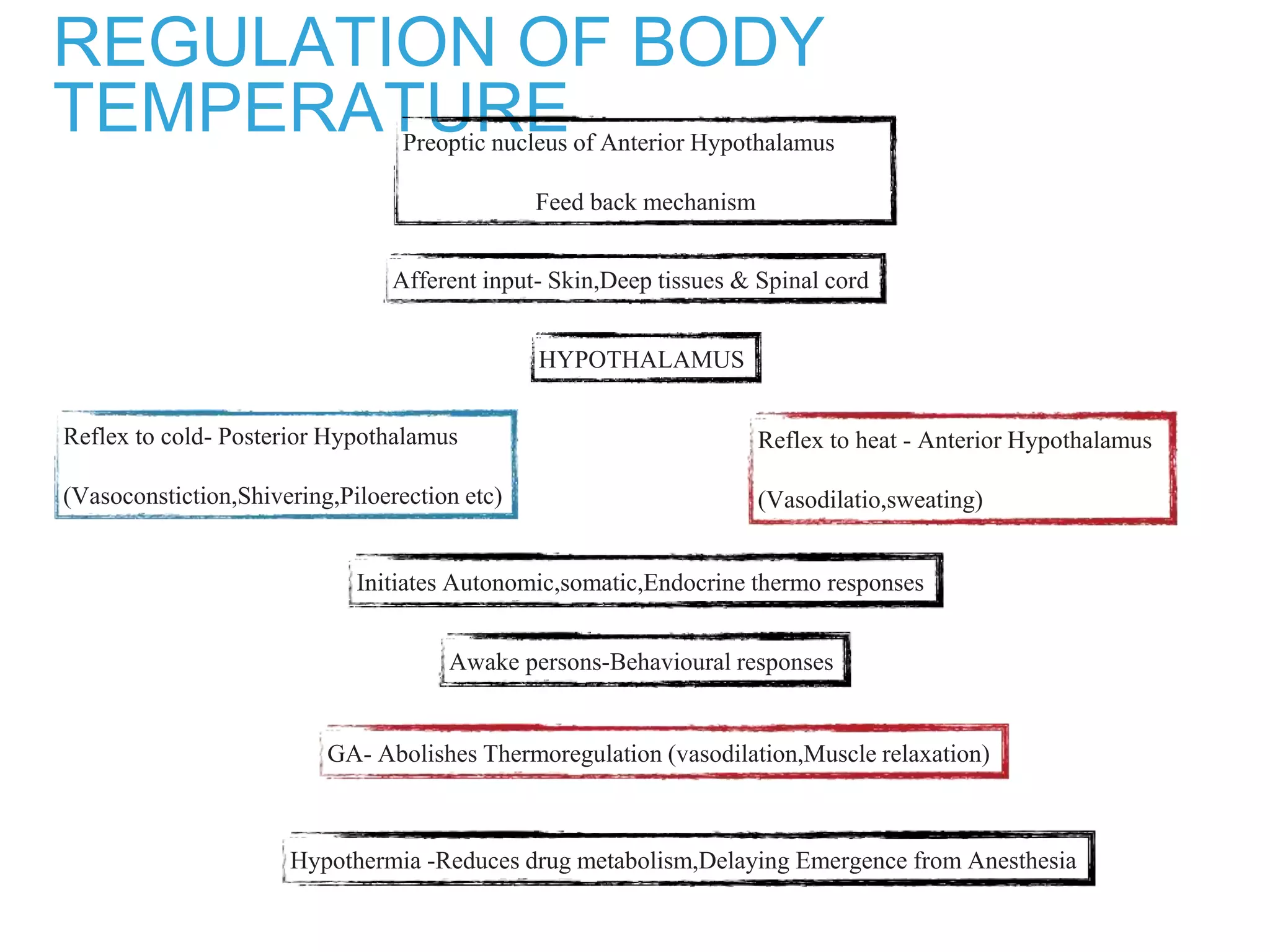
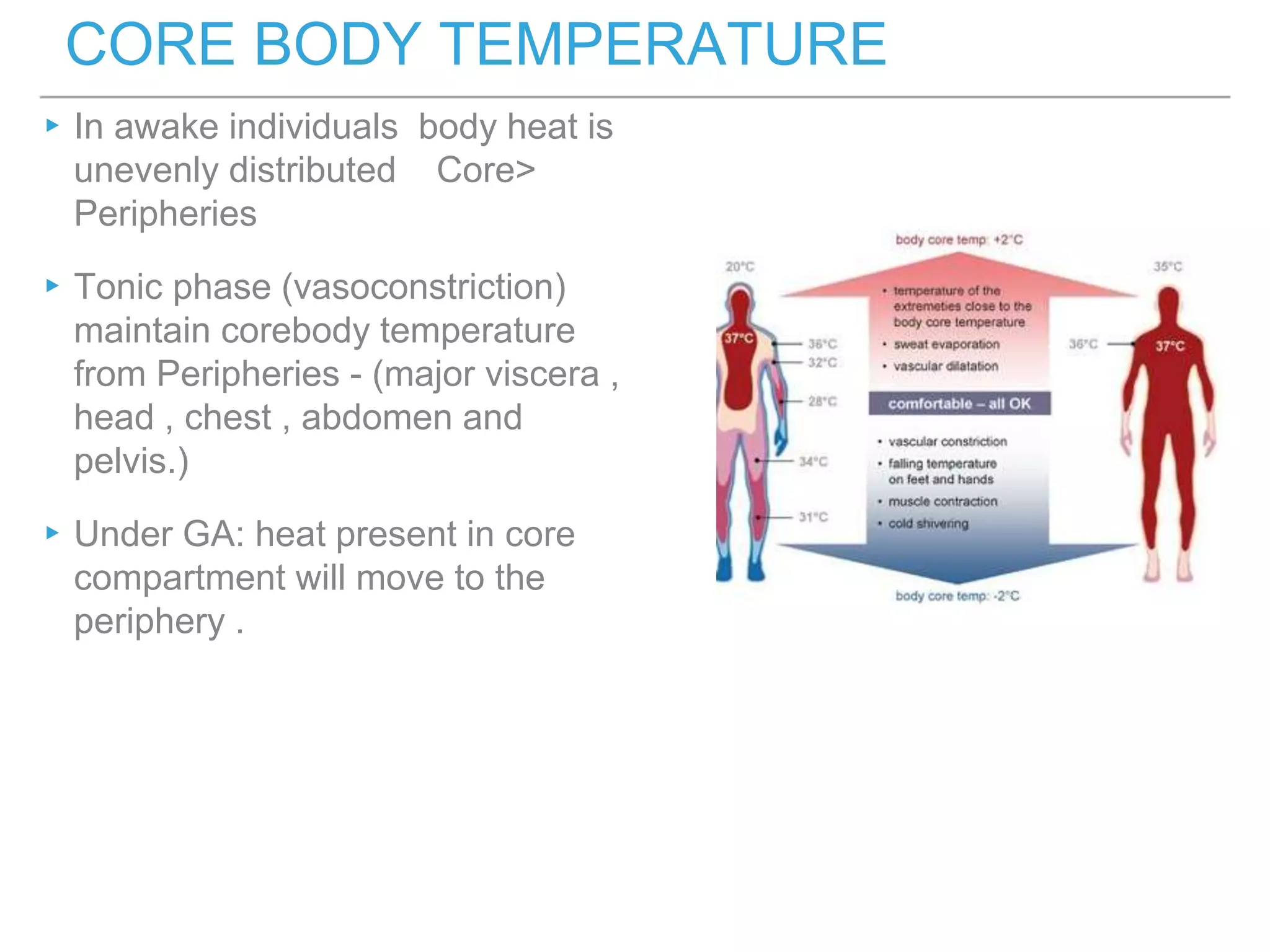
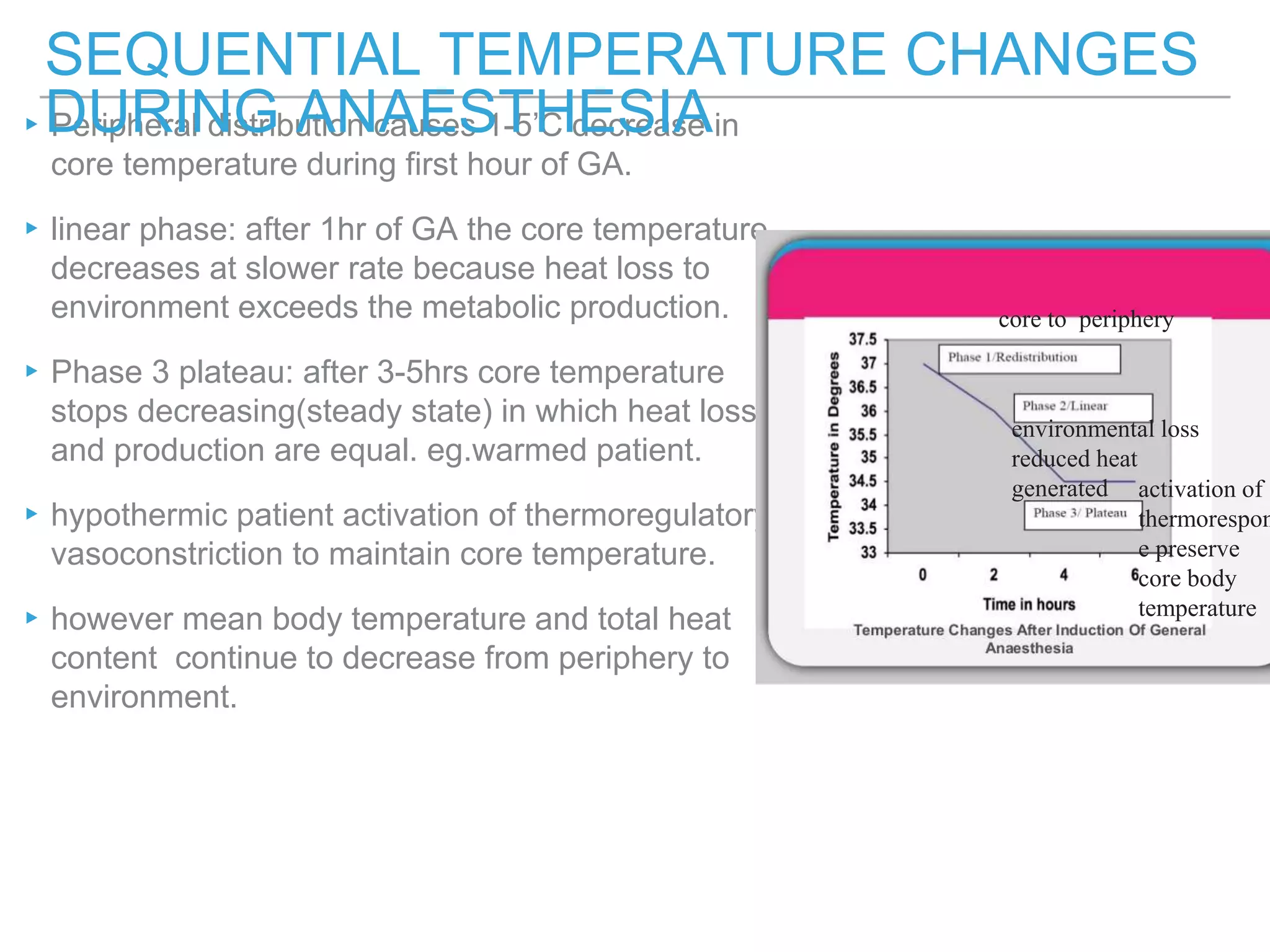
The document discusses thermoregulation and temperature monitoring. It summarizes that the hypothalamus regulates body temperature through heat production and loss mechanisms like radiation, conduction, convection, and evaporation. General anesthesia affects all aspects of thermoregulation by inhibiting responses like vasoconstriction and shivering that normally maintain core body temperature. This can lead to perioperative hypothermia if not prevented through measures like warmed fluids and surgical drapes.













































![TEMPERATURE REGULATION AND MONITORING.PPT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/trm1-250319181501-9a699d5f-thumbnail.jpg?width=640&height=640&fit=bounds)


















































