Downloaded 240 times



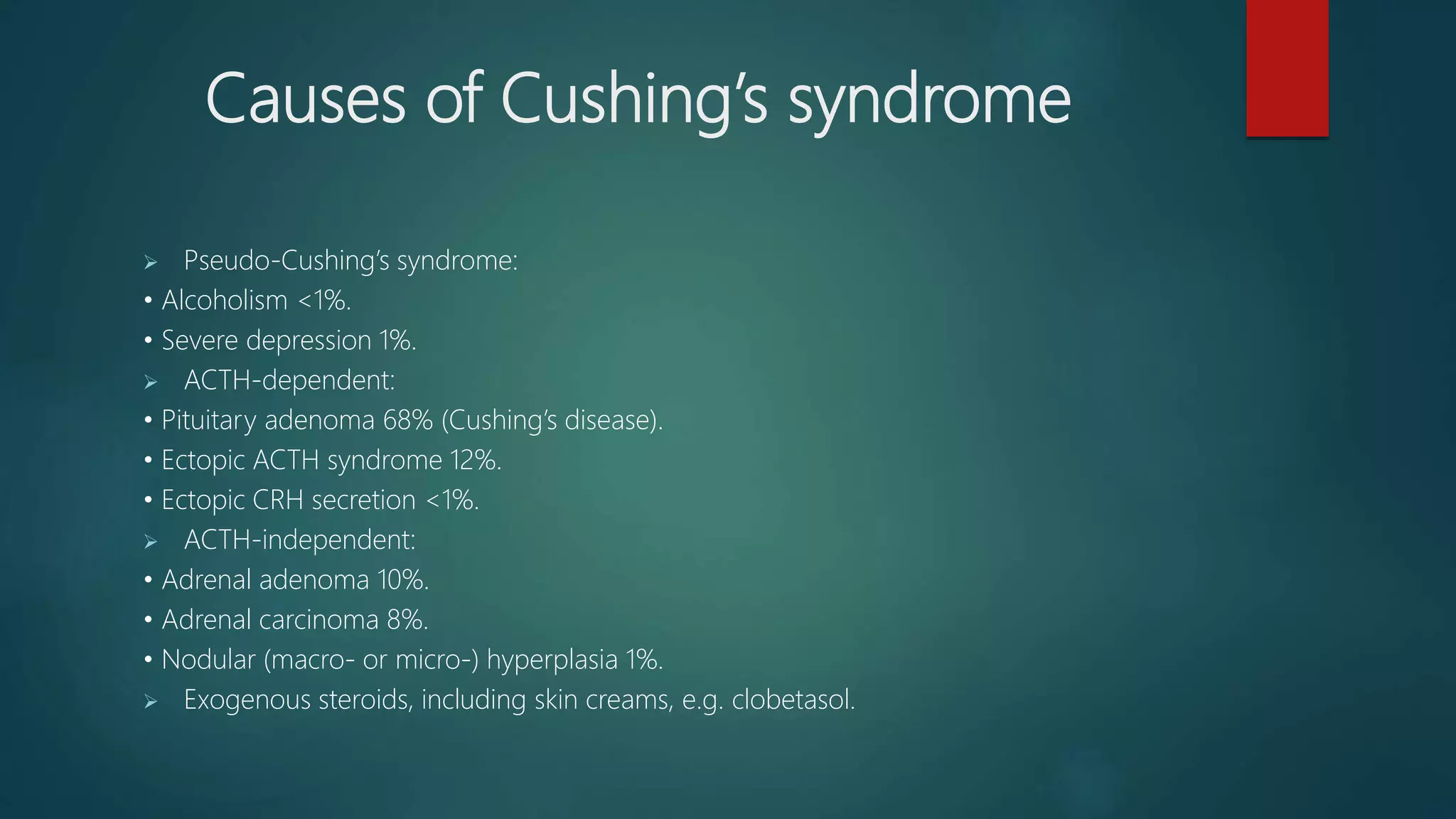







































This document provides information on Cushing's syndrome, including its definition, epidemiology, causes, clinical features, investigations, treatment, and follow-up. Cushing's syndrome results from excess cortisol secretion and can be fatal if left untreated. It is rare, affecting about 2 per million people annually. The causes include pituitary adenomas (68% of cases), ectopic ACTH secretion (12%), and adrenal tumors (18%). Clinical features include weight gain, high blood pressure, and mood disturbances. Investigations involve tests to evaluate cortisol levels and distinguish ACTH-dependent from independent causes. Treatment options are surgery, radiation, medication, and adrenalectomy. Follow-up aims to detect recurrence through monitoring cortisol





























































































