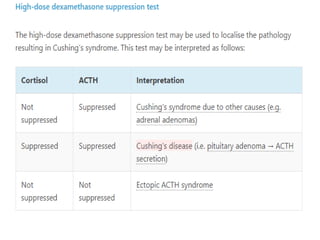
Cushing's syndrome results from chronic excess glucocorticoid exposure, leading to a range of symptoms like obesity, hypertension, and glucose intolerance, making diagnosis challenging. The condition has various causes, with iatrogenic Cushing's from glucocorticoid medications being the most common, particularly affecting women aged 25 to 45. Diagnosis involves several tests, including 24-hour urinary cortisol excretion and low-dose dexamethasone suppression tests, with treatment options ranging from surgical intervention to medication management depending on the underlying cause.



![Standard two-day 2 mg test.
• The two-day 2 mg test
• Administering 0.5 mg of dexamethasone every
six hours for eight doses.
• Measurement of serum (not urinary) cortisol
either two or six hours after the last dose.
• The same criteria for normal suppression (<1.8
mcg/dL [<50 nmol/L]) used as diagnostic.](https://image.slidesharecdn.com/cushingssyndrome-250112104551-555bca73/85/cushings-syndrome-topic-presentation-pptx-31-320.jpg)