Downloaded 35 times

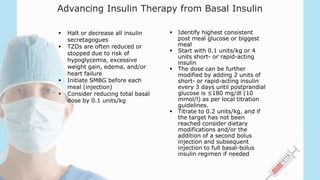
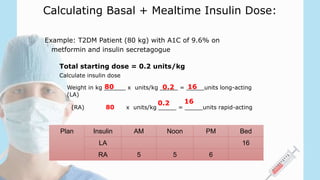
![Insulin Therapy Options
• Basal insulin only
• Bolus (Prandial) only
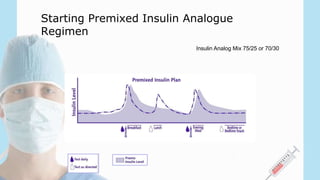
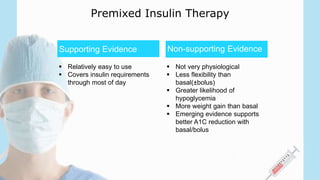
• Premixed
• Basal plus limited-meal bolus (‘Basal plus’)
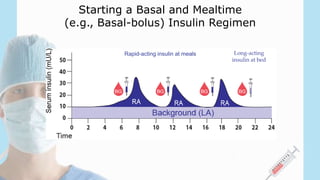
• Basal-Bolus (i.e. multiple daily injections - MDI)
• Basal-Bolus (i.e. continuous subcutaneous insulin infusion [CSII],
“Insulin Pump”)](https://image.slidesharecdn.com/diabetesinclinicalpractice2-151003194930-lva1-app6891/85/Diabetes-in-clinical-practice2-7-320.jpg)
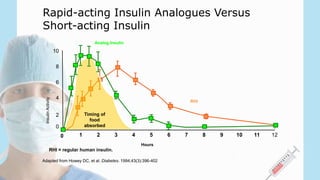
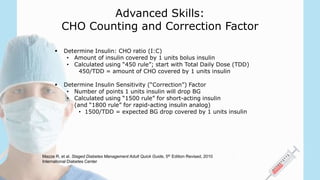
![Sequential Insulin Strategies in T2DM
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of
print]
Management of Hyperglycemia in Type 2 Diabetes:
Sequential Insulin Strategies](https://image.slidesharecdn.com/diabetesinclinicalpractice2-151003194930-lva1-app6891/85/Diabetes-in-clinical-practice2-18-320.jpg)
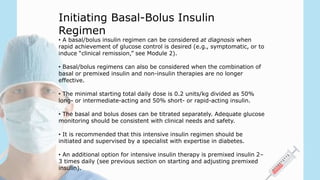
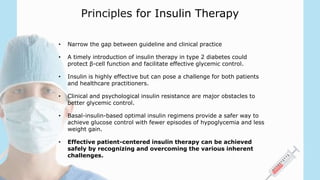
![Advancing Basal Insulin
If most AM fasting BG
>120 mg/dL
(>6.7 mmol/L)
Titrate until fasting glucose at target BG
• Increase 2 units [or 4 units if FBG >180
mg/dl or 10 mmol/L] every 3 days
• If dose reaches ~0.5 units/kg body weight,
consider adding mealtime insulin
If most AM fasting BG
<120 mg/dL
(<6.7 mmol/L) and
A1C remains above target
Test pre–evening meal and bedtime
(or 2-hour post–evening meal) and consider
need for mealtime insulin
If hypoglycemia or FPG
< 70 mg/dL
Reduce insulin dose by 3 units or 10%,
whichever is greater](https://image.slidesharecdn.com/diabetesinclinicalpractice2-151003194930-lva1-app6891/85/Diabetes-in-clinical-practice2-23-320.jpg)

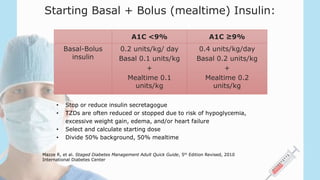
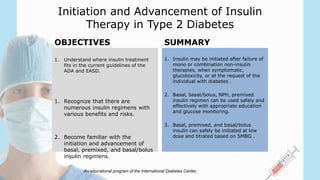


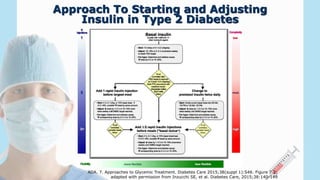
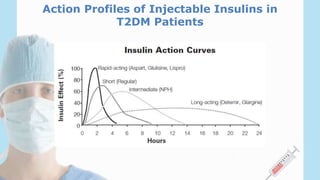
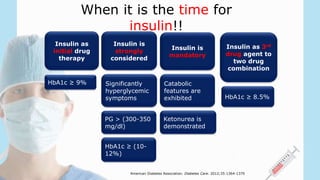
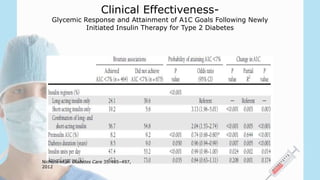
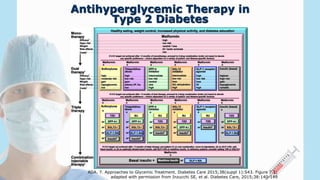
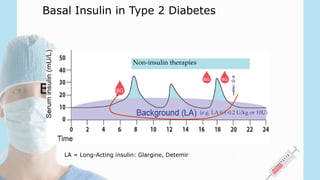
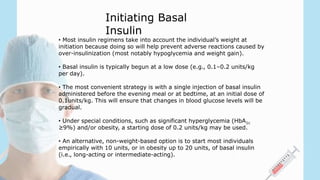
1) Insulin therapy is recommended for type 2 diabetes patients with an HbA1c ≥9%, significant hyperglycemia, or when other treatments fail to control blood glucose levels. 2) There are several options for insulin therapy including basal insulin only, premixed insulin, or basal-bolus regimens. Basal insulin aims to provide background insulin levels while bolus insulin covers mealtime spikes. 3) When initiating insulin, it is important to assess the patient's needs, educate them on self-monitoring, and start at a low dose such as 0.1-0.2 units/kg of basal insulin daily to minimize risks of hypoglycemia and weight gain. The dose is then gradually



































































