Downloaded 908 times



![References
Nursing Crib (2008). Cushing’s Syndrome, The
Student Nurses Comment, On line [Accessed on
12.06.2009: 16:25Hrs],
http://nursingcrib.com/category/nursing-notes-
reviewer/medical-surgical-nursing/
PNT Students - Gertrude's Gardens Children's Hospital (2009) 05/07/09 50](https://image.slidesharecdn.com/cushingssyndrome-090705095633-phpapp02/85/Cushings-Syndrome-50-320.jpg)

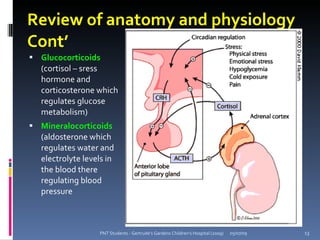
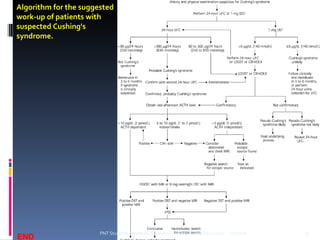
The document provides objectives and an overview of Cushing's syndrome, including its aetiology, pathophysiology, clinical manifestations, diagnosis, and nursing management. It aims to equip nursing students with knowledge of Cushing's syndrome and the management of a child presenting with the disorder through increased cortisol levels. A case study is presented to demonstrate nursing assessments and diagnoses for a teenage girl diagnosed with Cushing's syndrome.



































































