Download as PDF, PPTX
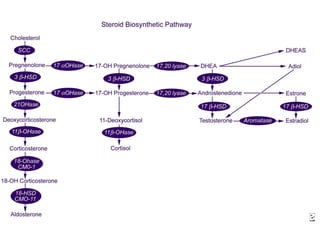
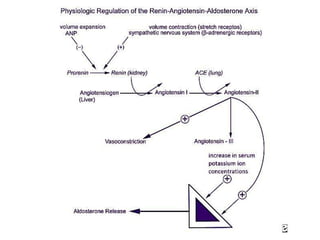



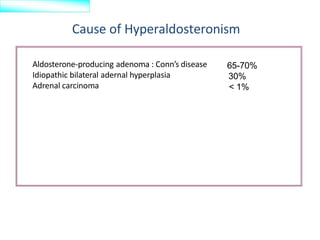





1) Primary hyperaldosteronism, also known as Conn's syndrome, is characterized by excessive secretion of the hormone aldosterone from the adrenal glands, causing increased sodium retention and potassium excretion. 2) It can be caused by an aldosterone-producing adenoma, idiopathic bilateral adrenal hyperplasia, or adrenal carcinoma. Aldosterone-producing adenomas account for 65-70% of cases. 3) Symptoms include hypertension, hypokalemia, headaches, and muscle weakness. Diagnostic tests include measuring aldosterone and renin levels, with an elevated aldosterone-to-renin ratio confirming the diagnosis. Treatment options include surgical removal of





























![Hyperaldosteronism new[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hyperaldosteronismnew1-120226175449-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























































