Downloaded 464 times


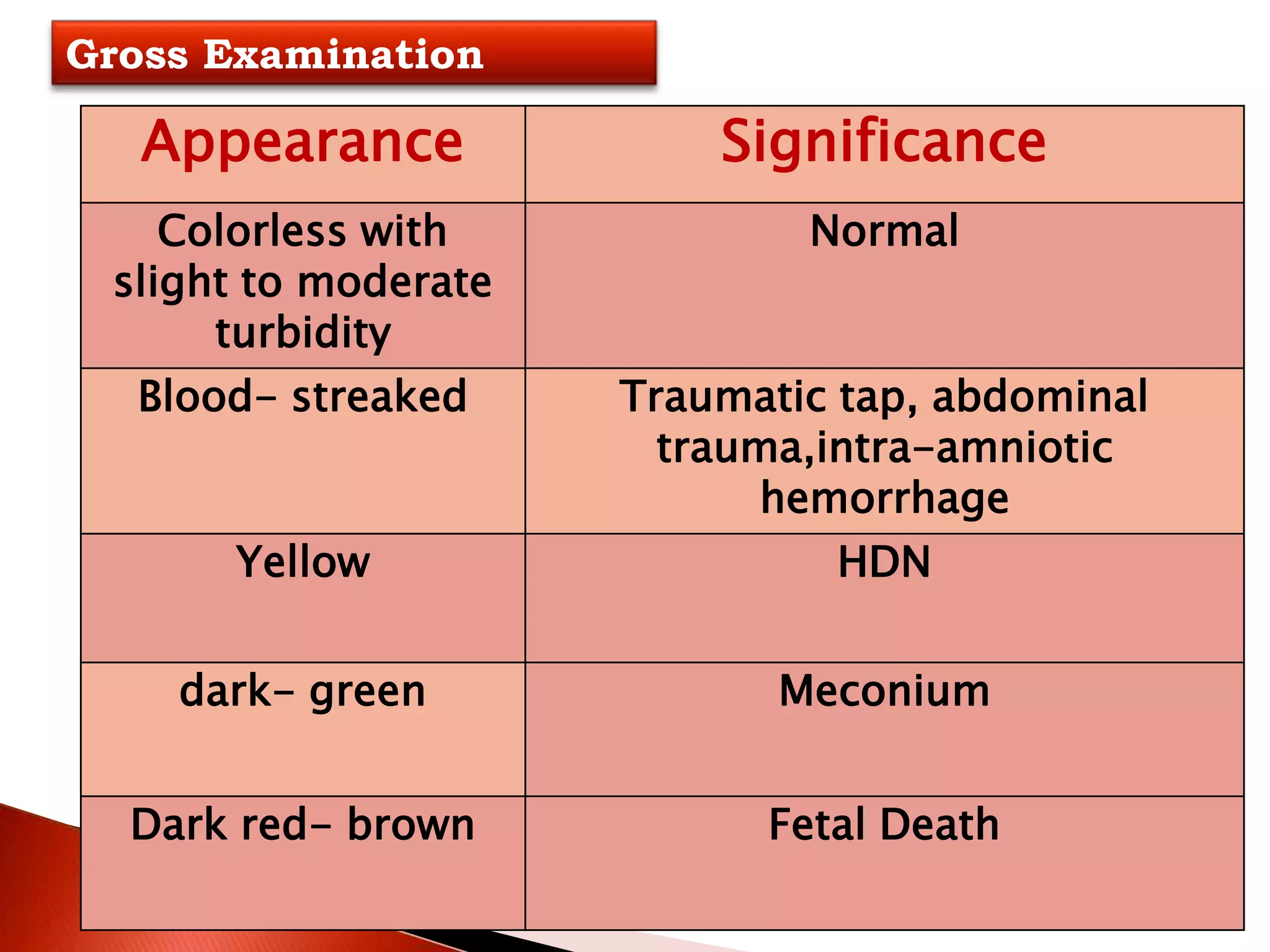
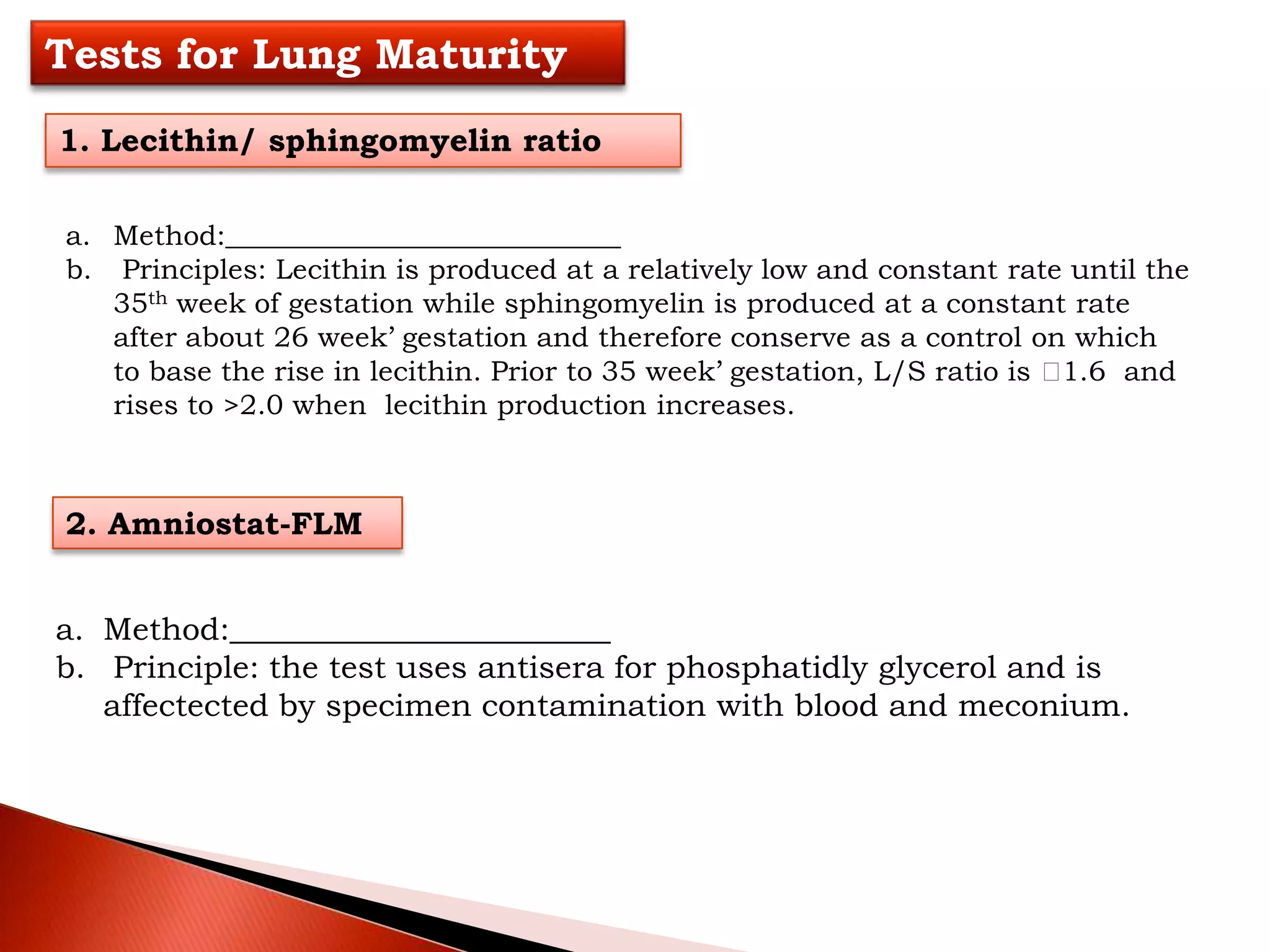






Amniotic fluid provides protection and nutrients for the developing fetus. Analysis of amniotic fluid obtained through amniocentesis can be used to assess fetal lung maturity, detect fetal distress, and screen for genetic and infectious disorders. Tests of amniotic fluid measure surfactant levels, bilirubin levels, and concentrations of proteins like alpha-fetoprotein to evaluate lung development and identify issues like hemorrhage or neural tube defects. Precise collection and rapid processing of amniotic fluid specimens is important for obtaining accurate test results.






















































