Downloaded 300 times

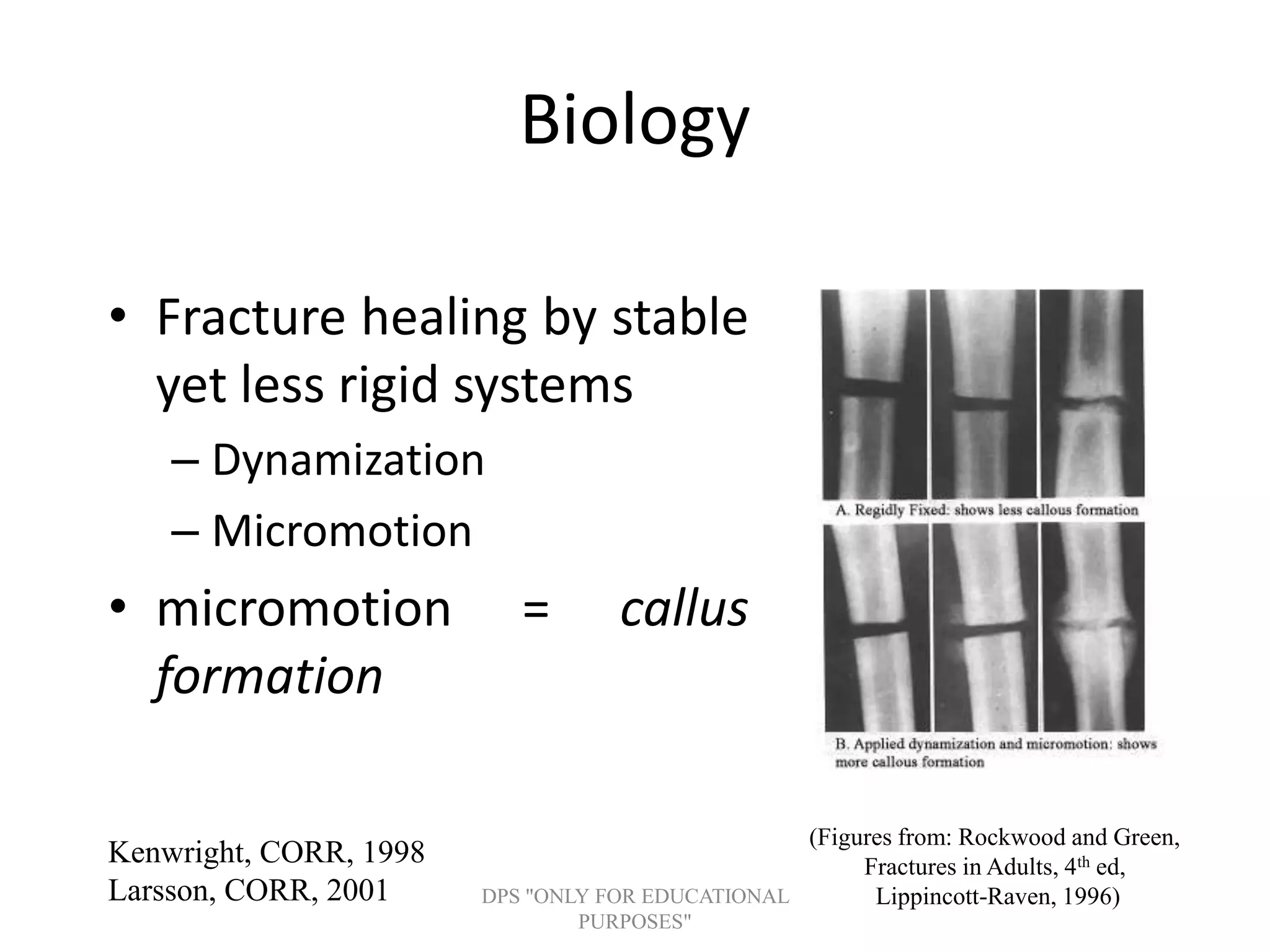


External fixation is used for definitive or temporary treatment of fractures. It has advantages of being minimally invasive and flexible, but disadvantages include potential pin site infections, inadequate immobilization, and soft tissue complications. Key components are pins, clamps, and connecting rods or rings. Pins must be carefully placed to avoid neurovascular injury and ensure stability. Frame construction and pin placement principles maximize stability and load sharing to promote fracture healing. Conversion to internal fixation is generally safe if done within 2-3 weeks to prevent pin track infections from compromising outcomes.
Introduction to external fixation principles, including overview of key topics: indications, advantages, disadvantages, mechanics, biology, and complications.
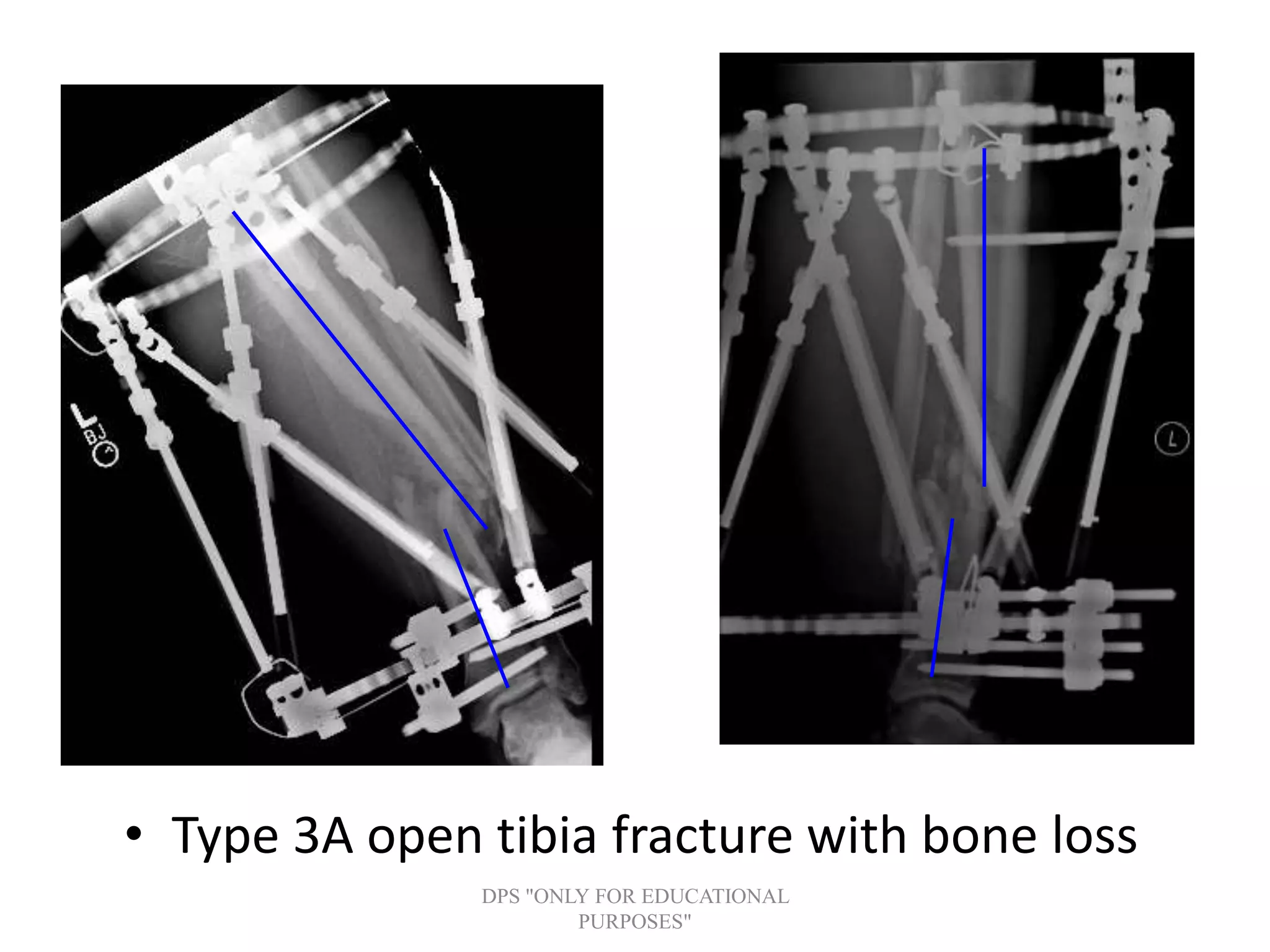
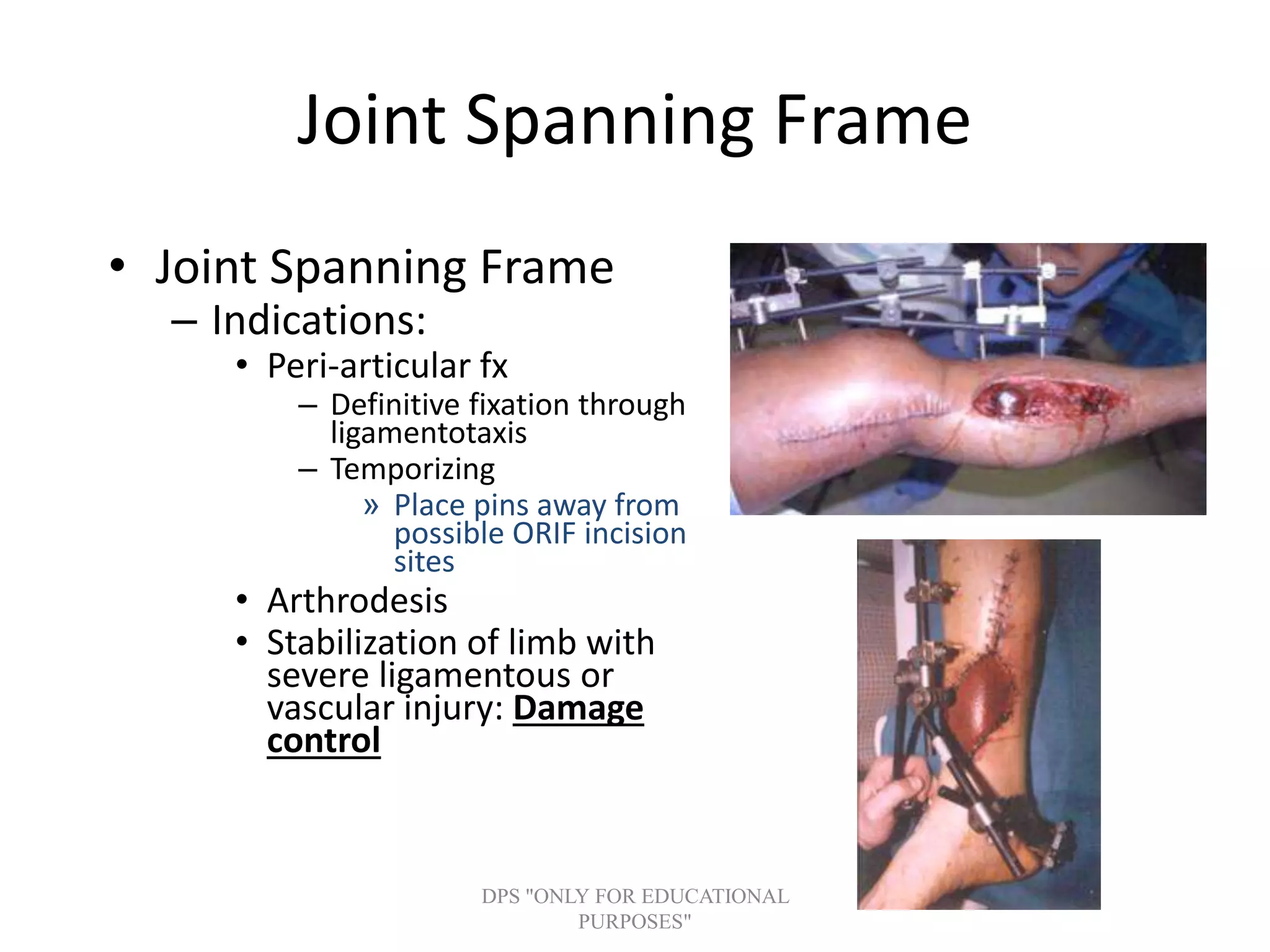
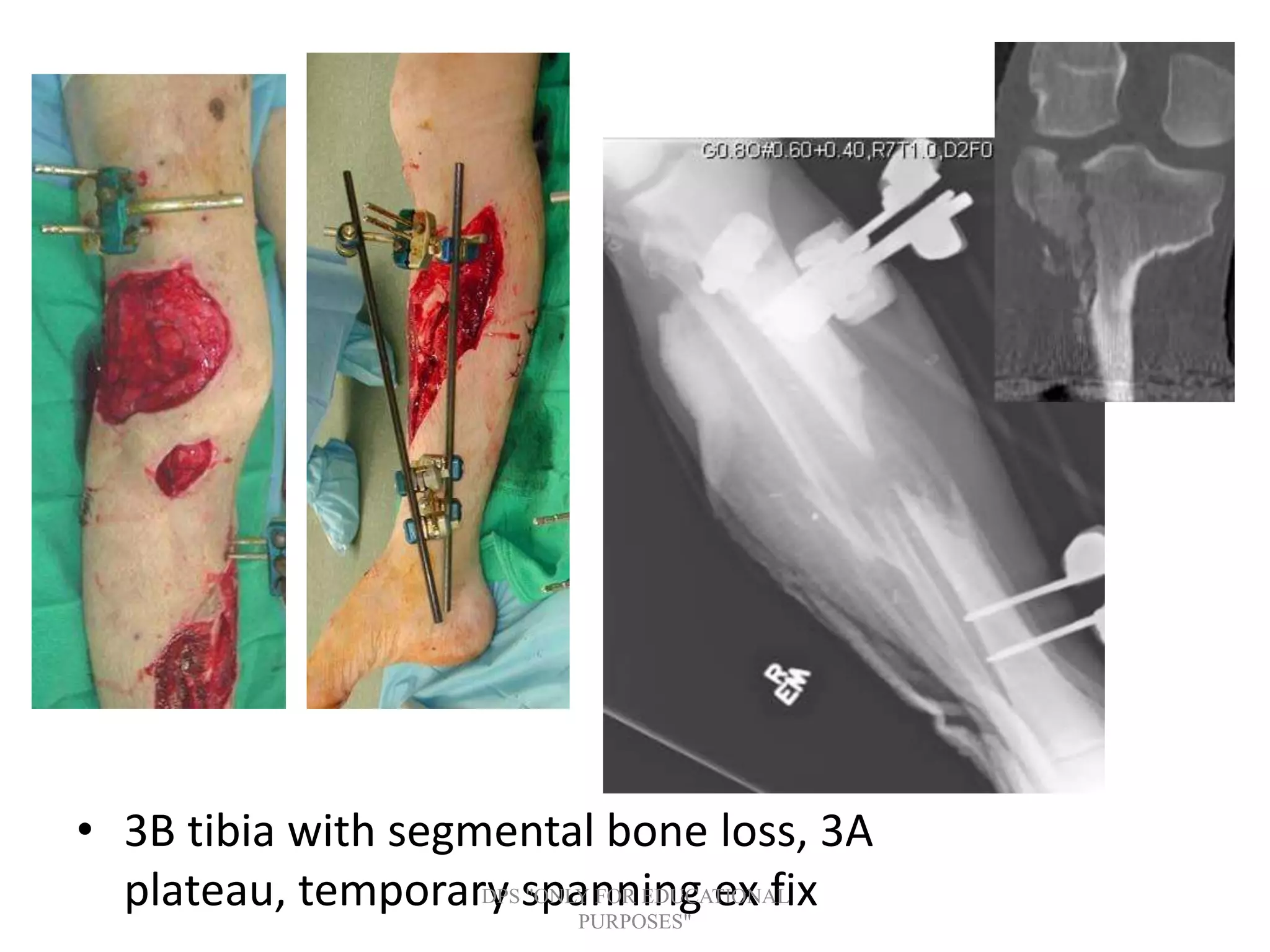
Definitive and temporary fixation indications, including fractures like open and peri-articular, and conditions like malunion, osteomyelitis, limb deformity.
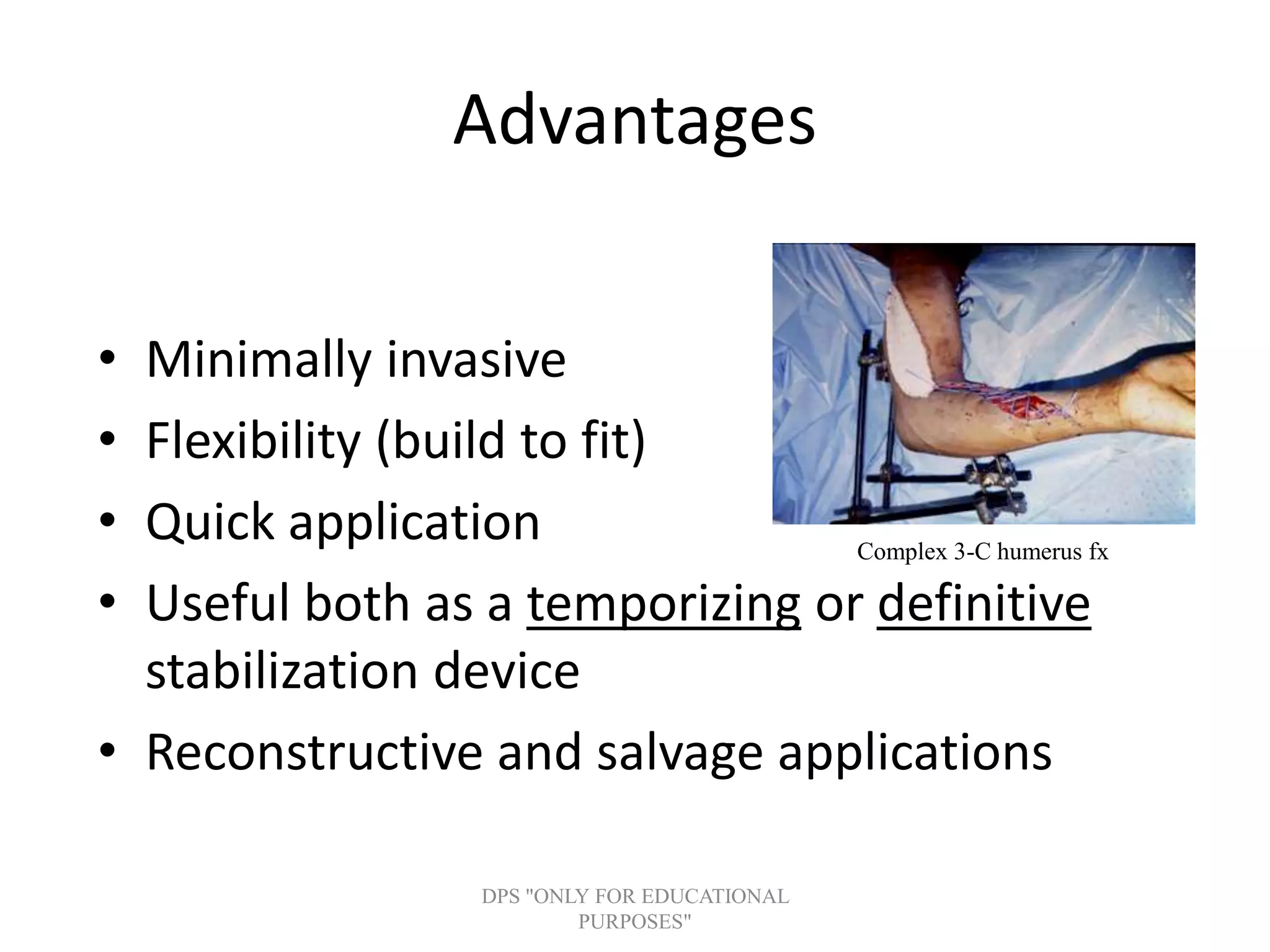
Key benefits of external fixation: minimally invasive, flexible, quick application, useful for stabilization, and reconstructive applications.
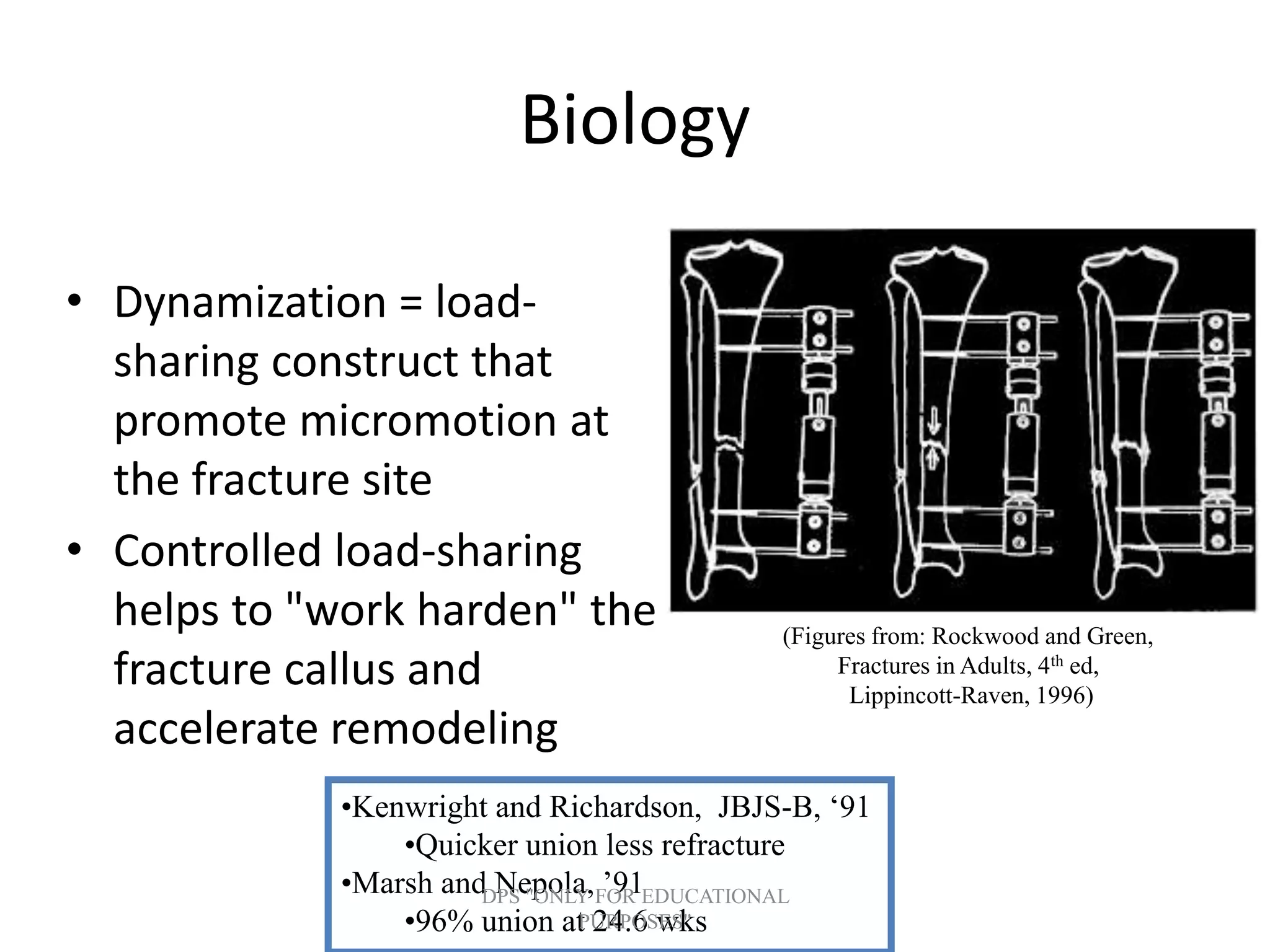
Major drawbacks include mechanical issues (like distraction) and biological risks (like infection), causing potential malunion or loss of function.
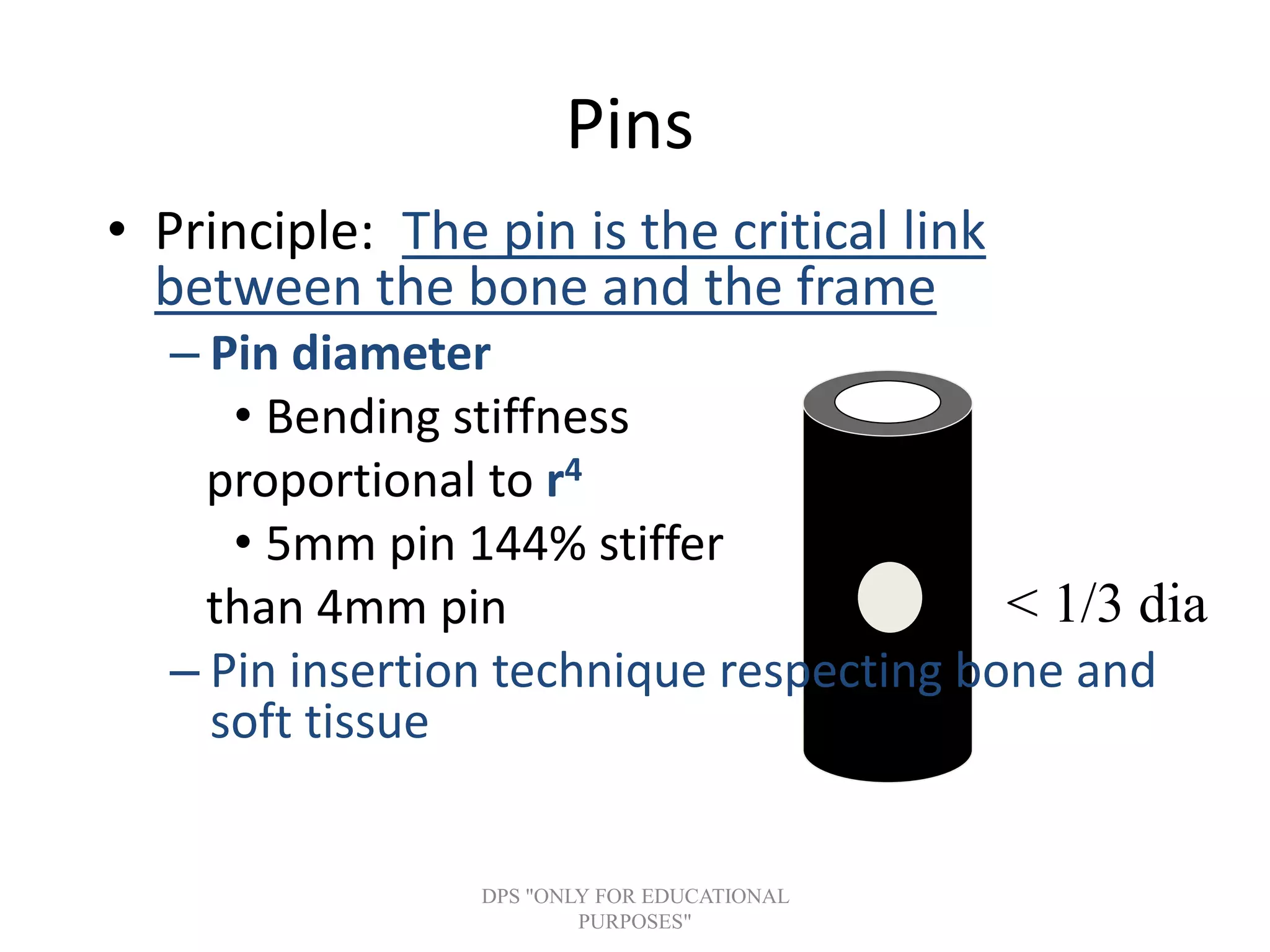
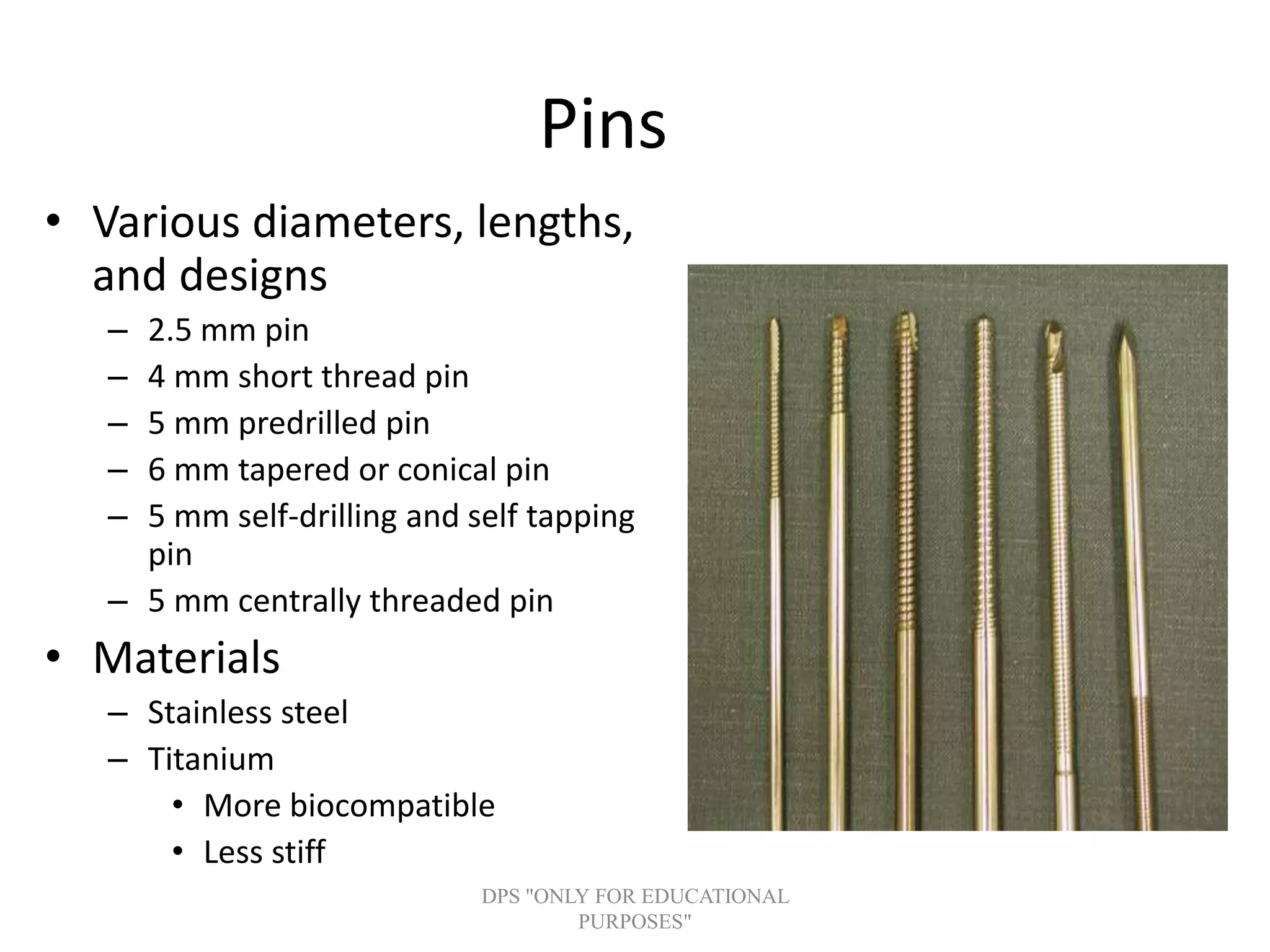
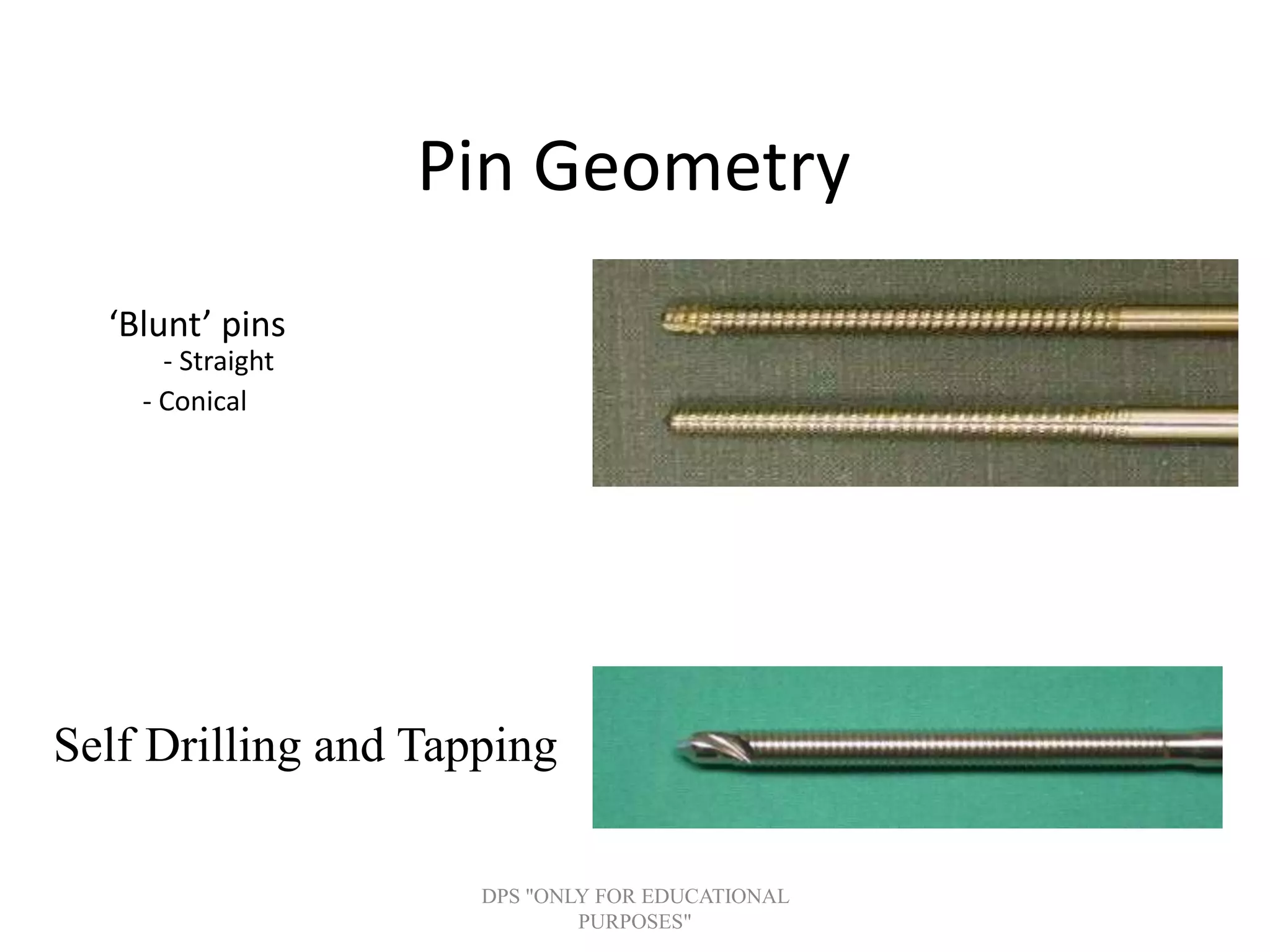
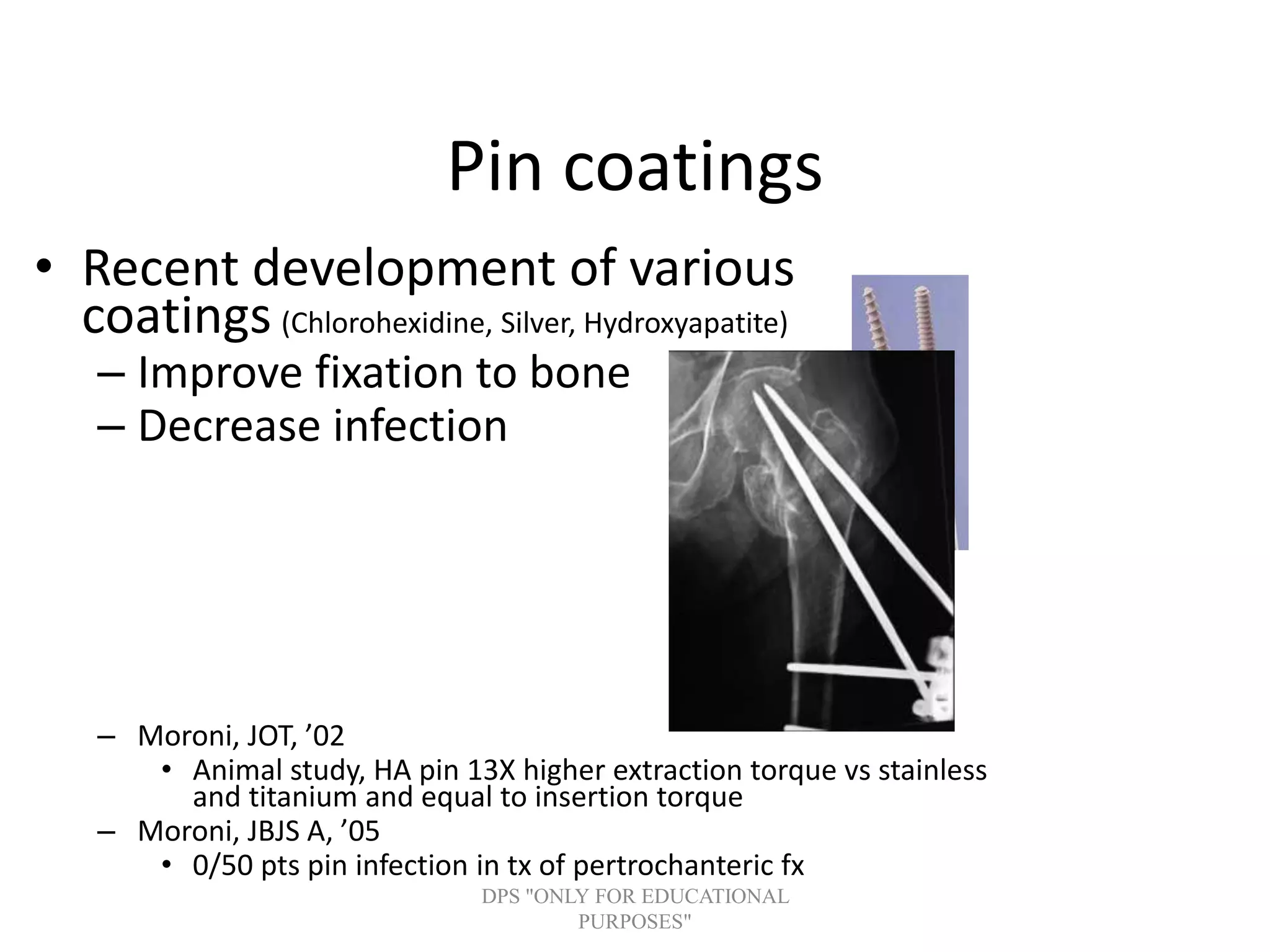
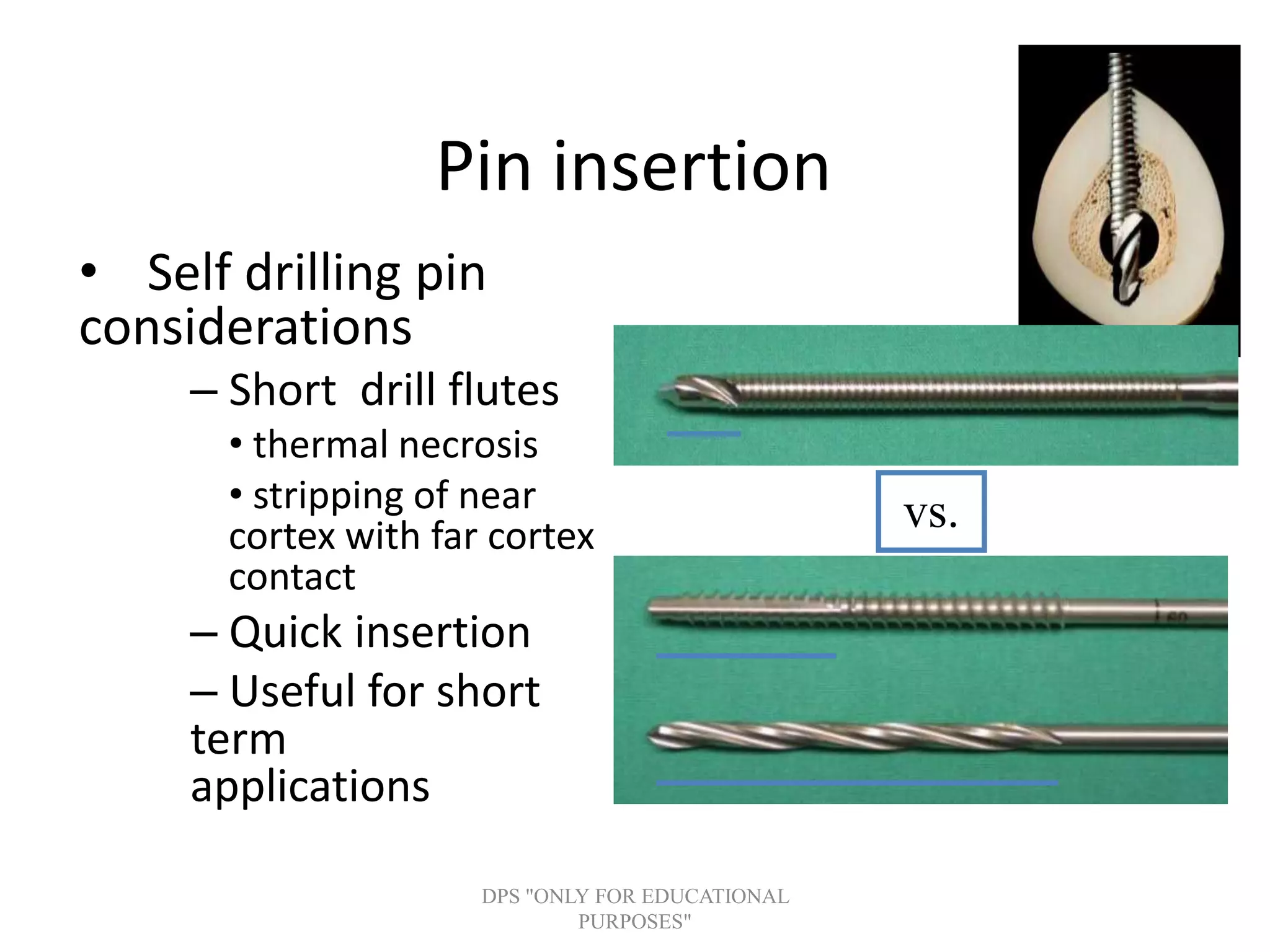
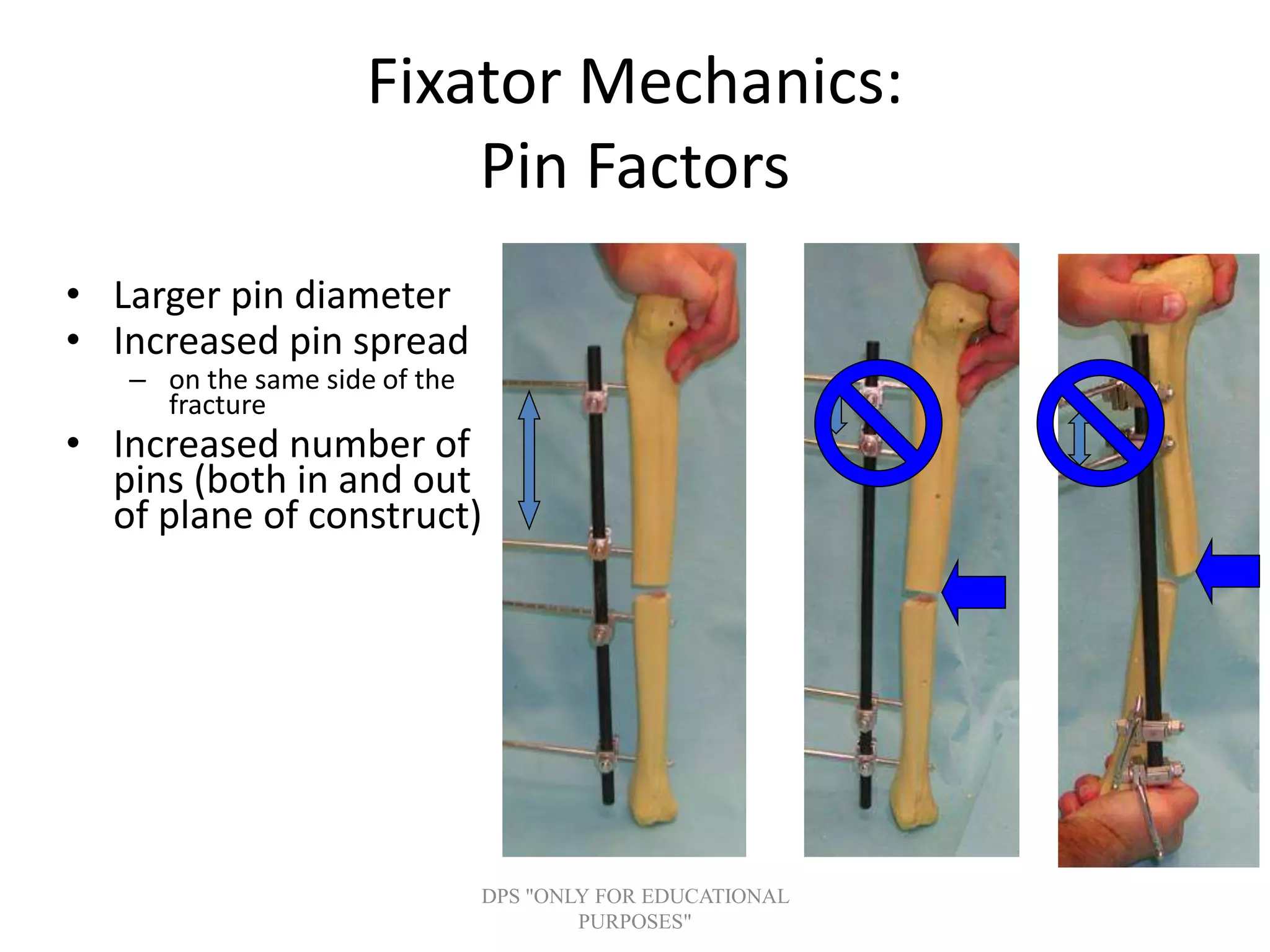
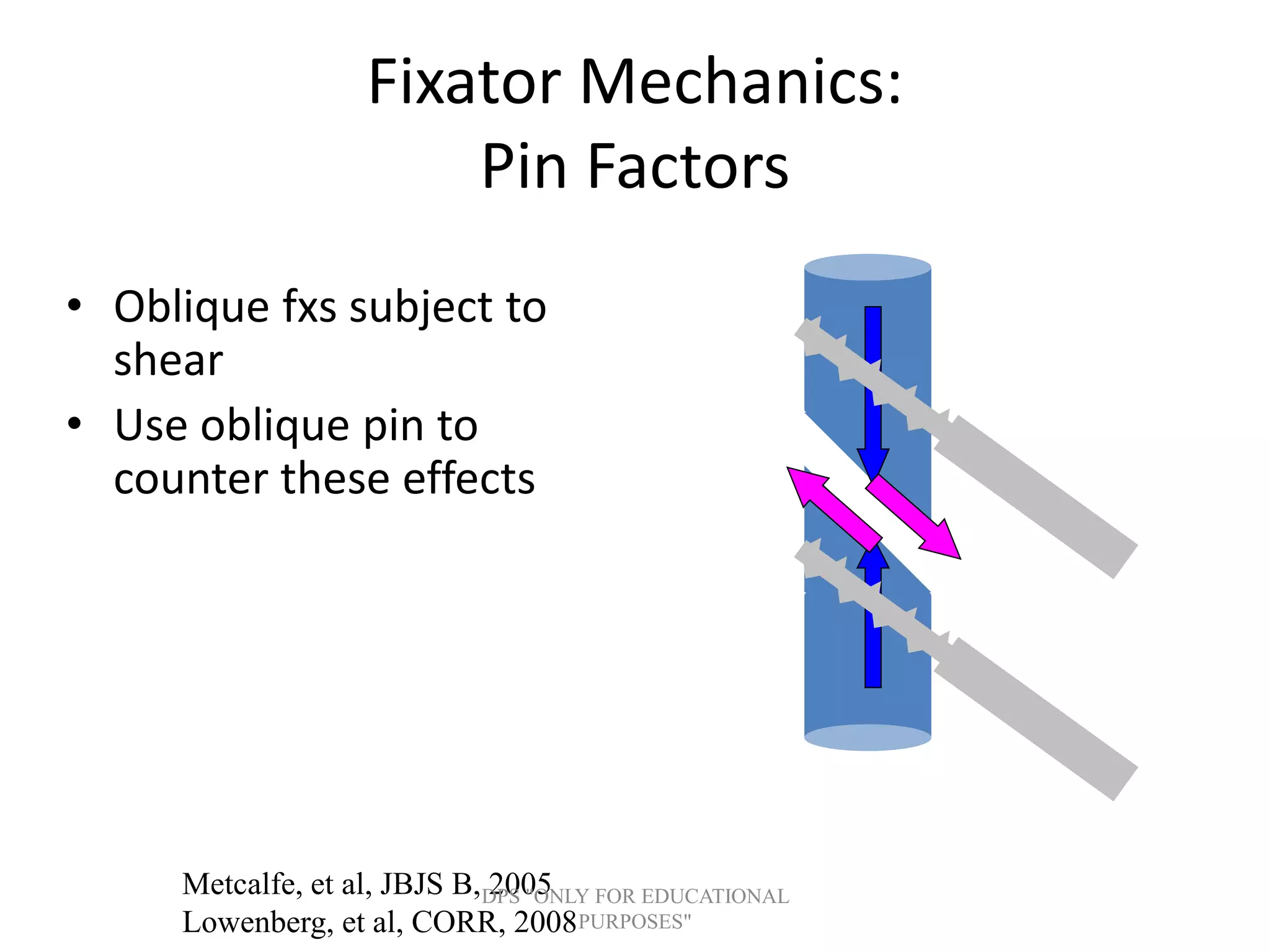
Overview and details on components such as pins (various types and diameters), their geometry, and advancements in coatings to improve stability and reduce infections.
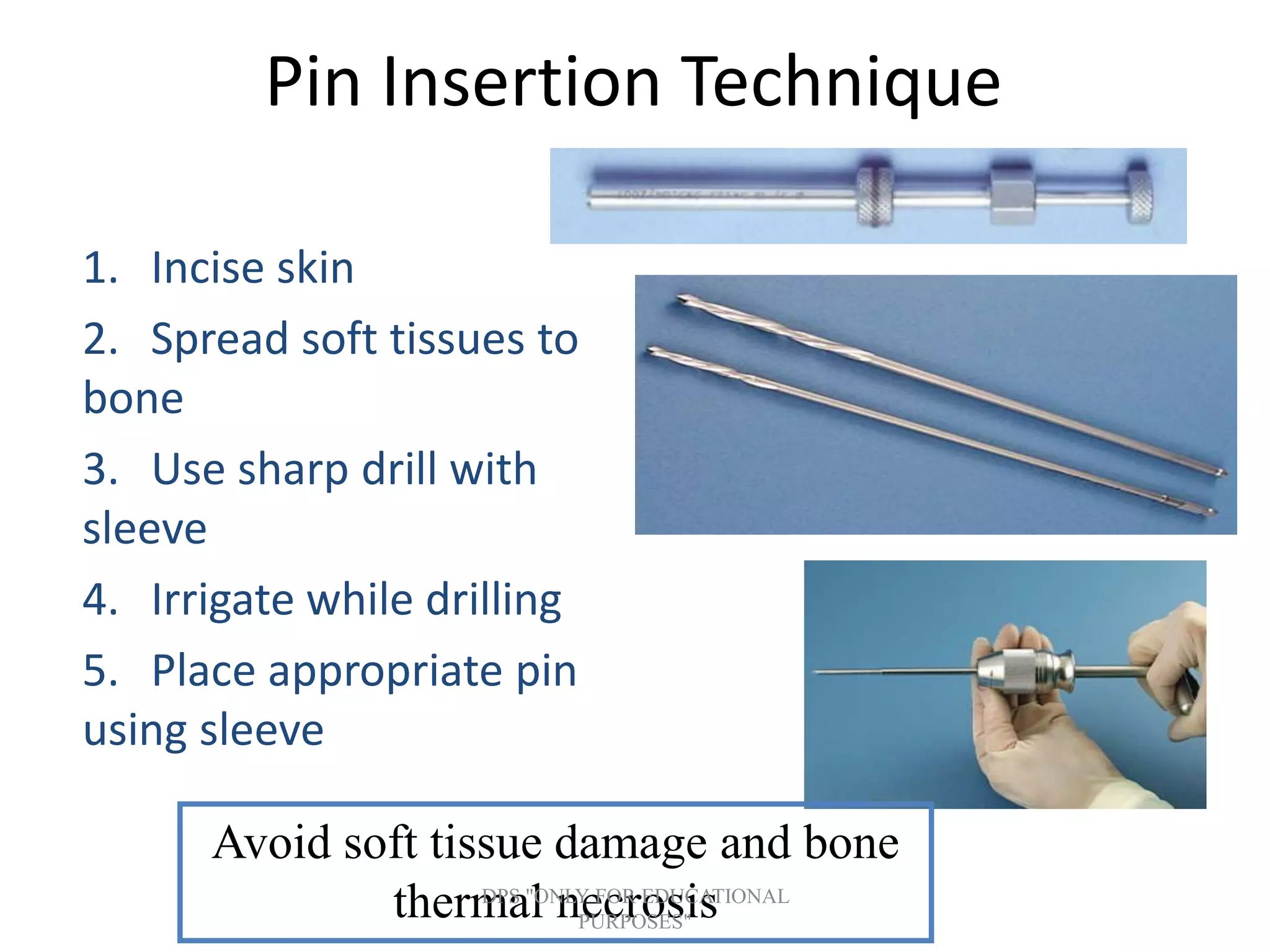
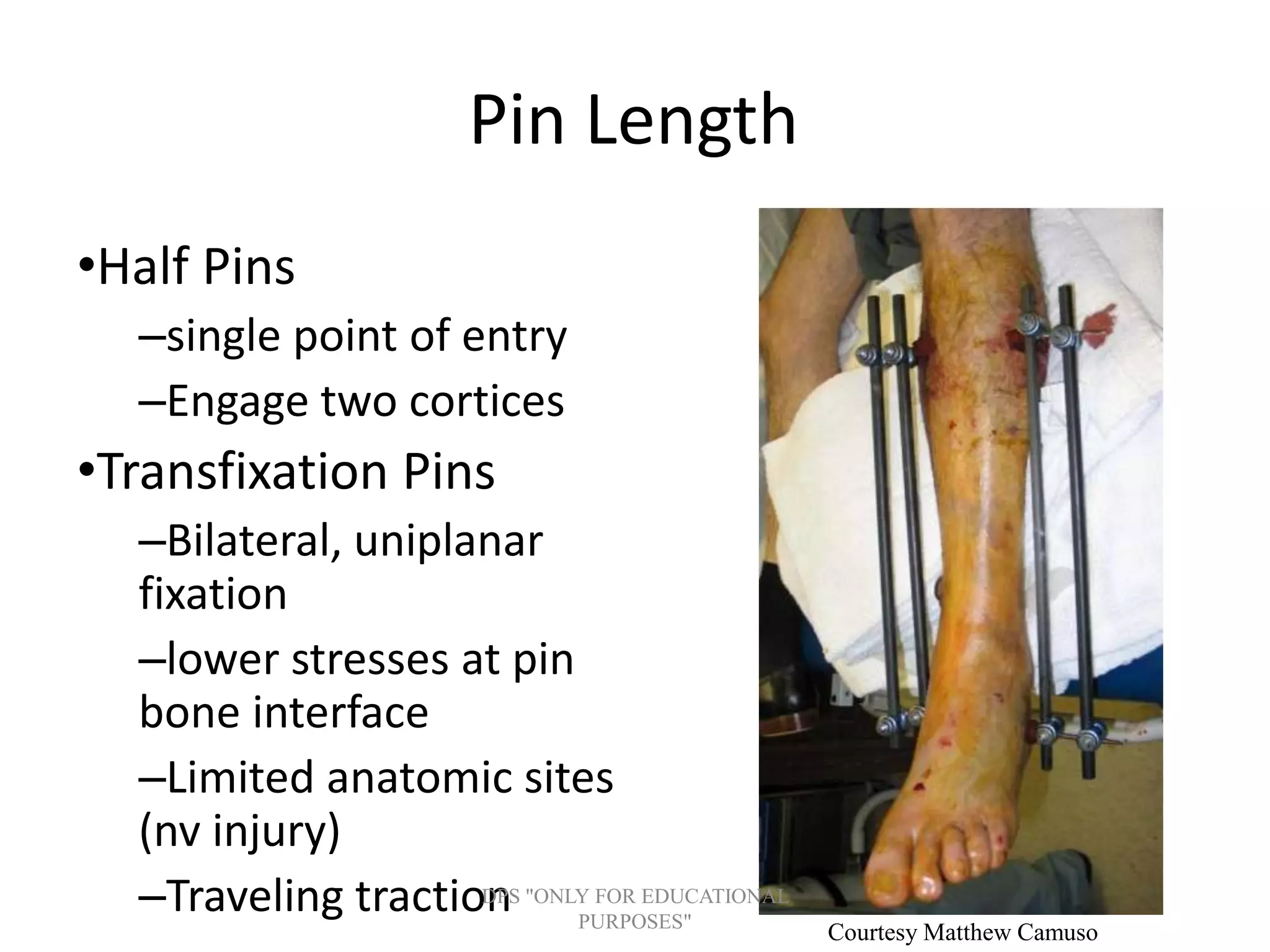
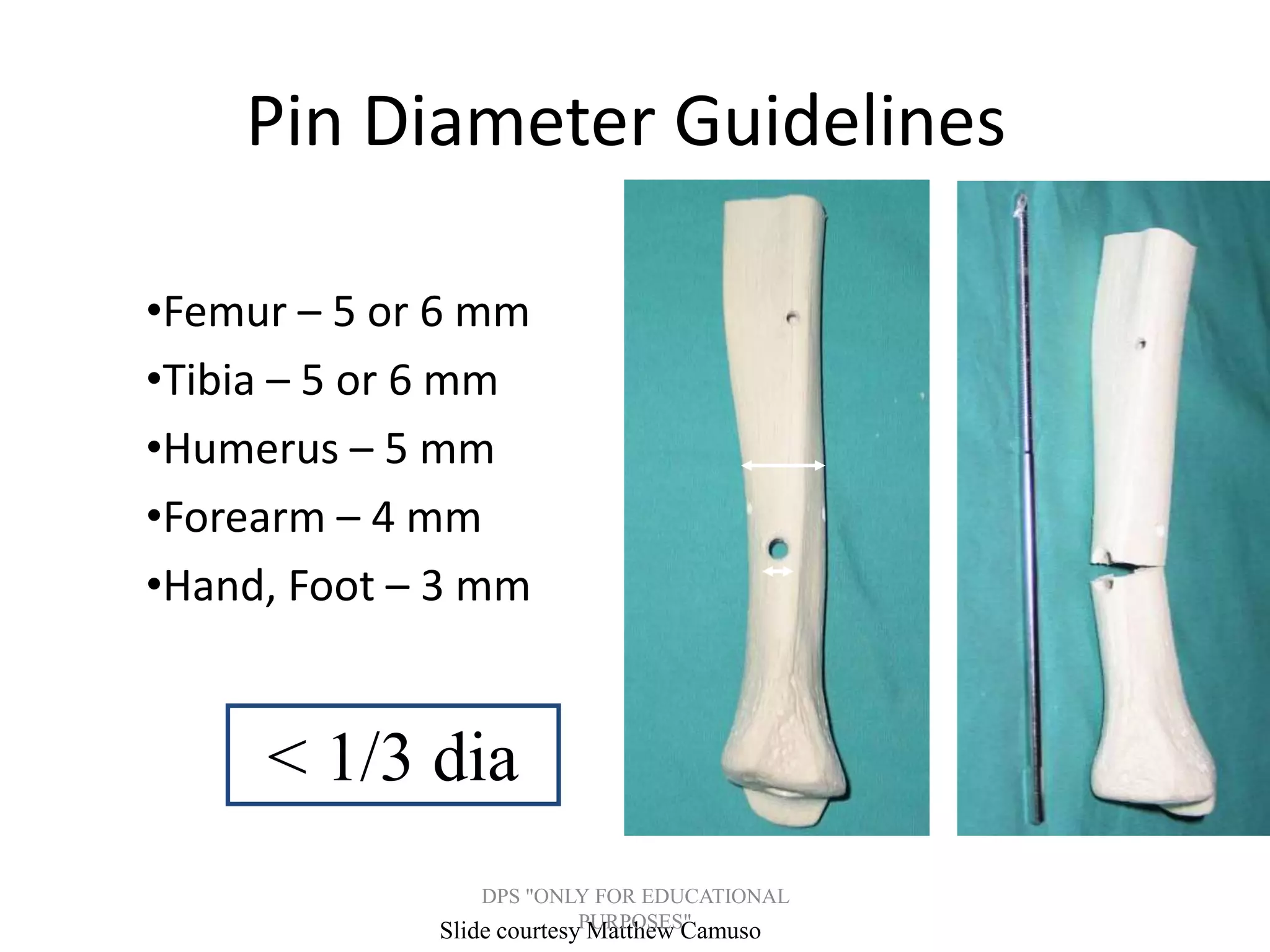
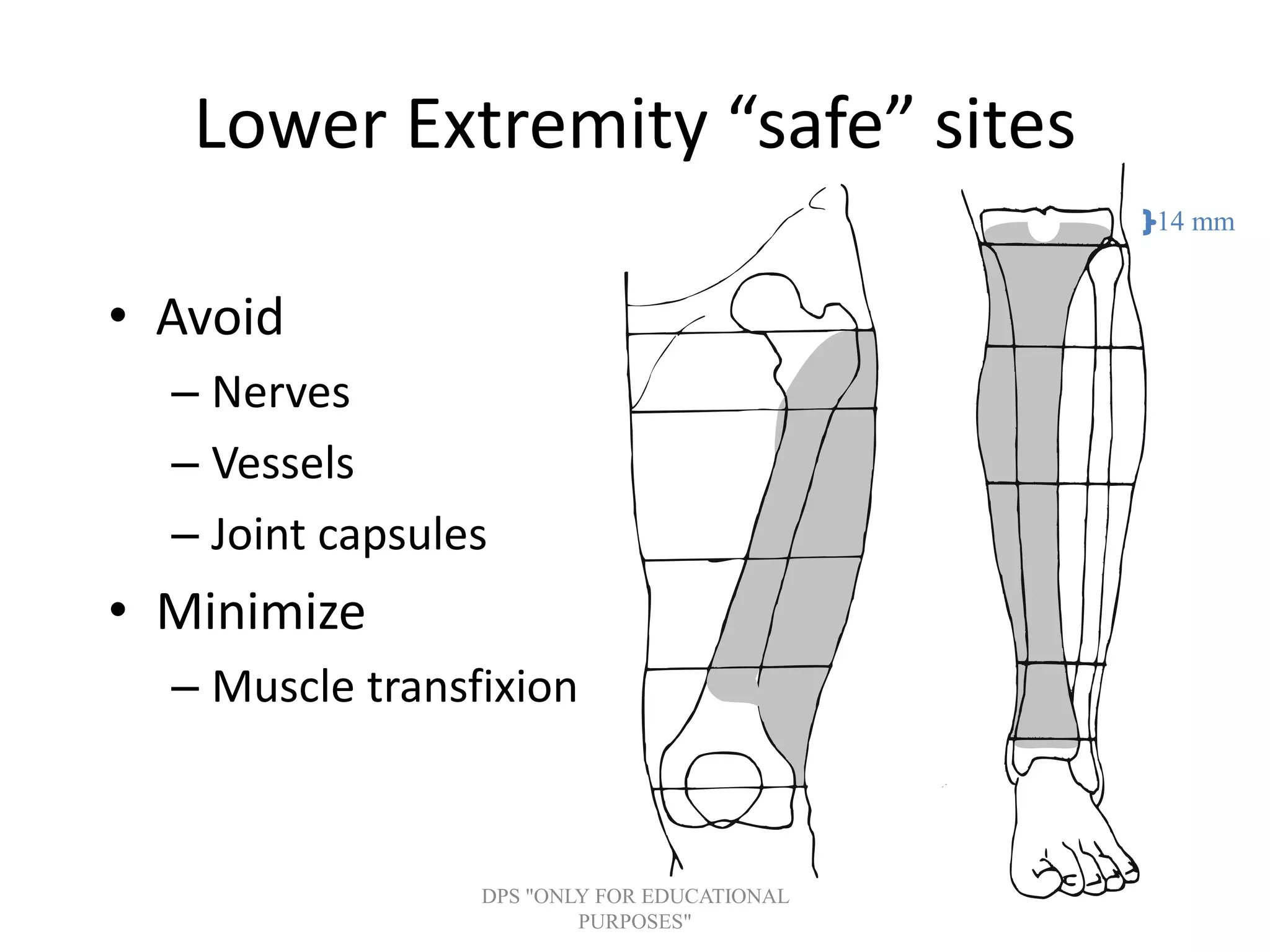
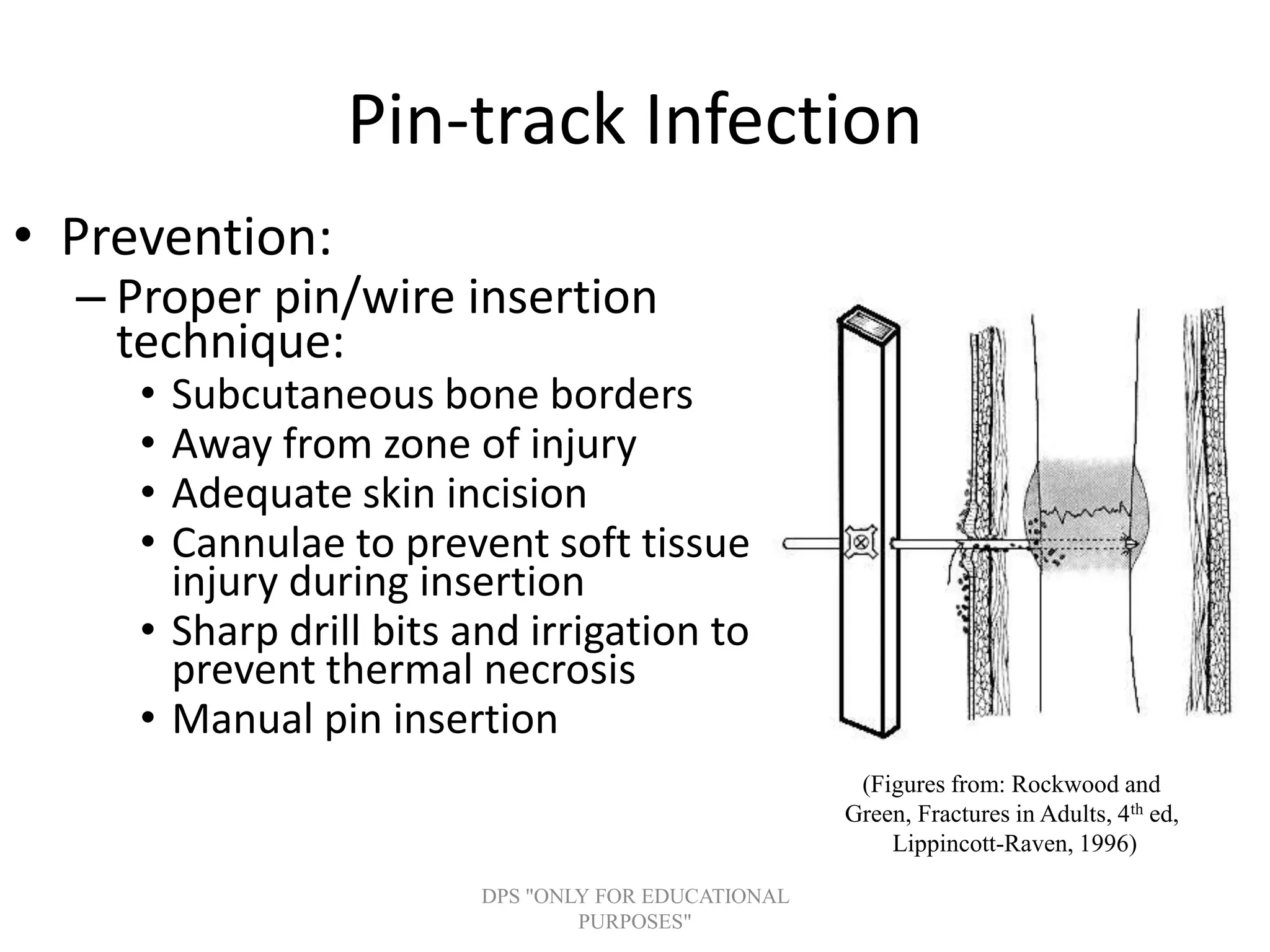
Methods and guidelines for proper pin insertion techniques, addressing pin length and diameter guidelines for various bones.
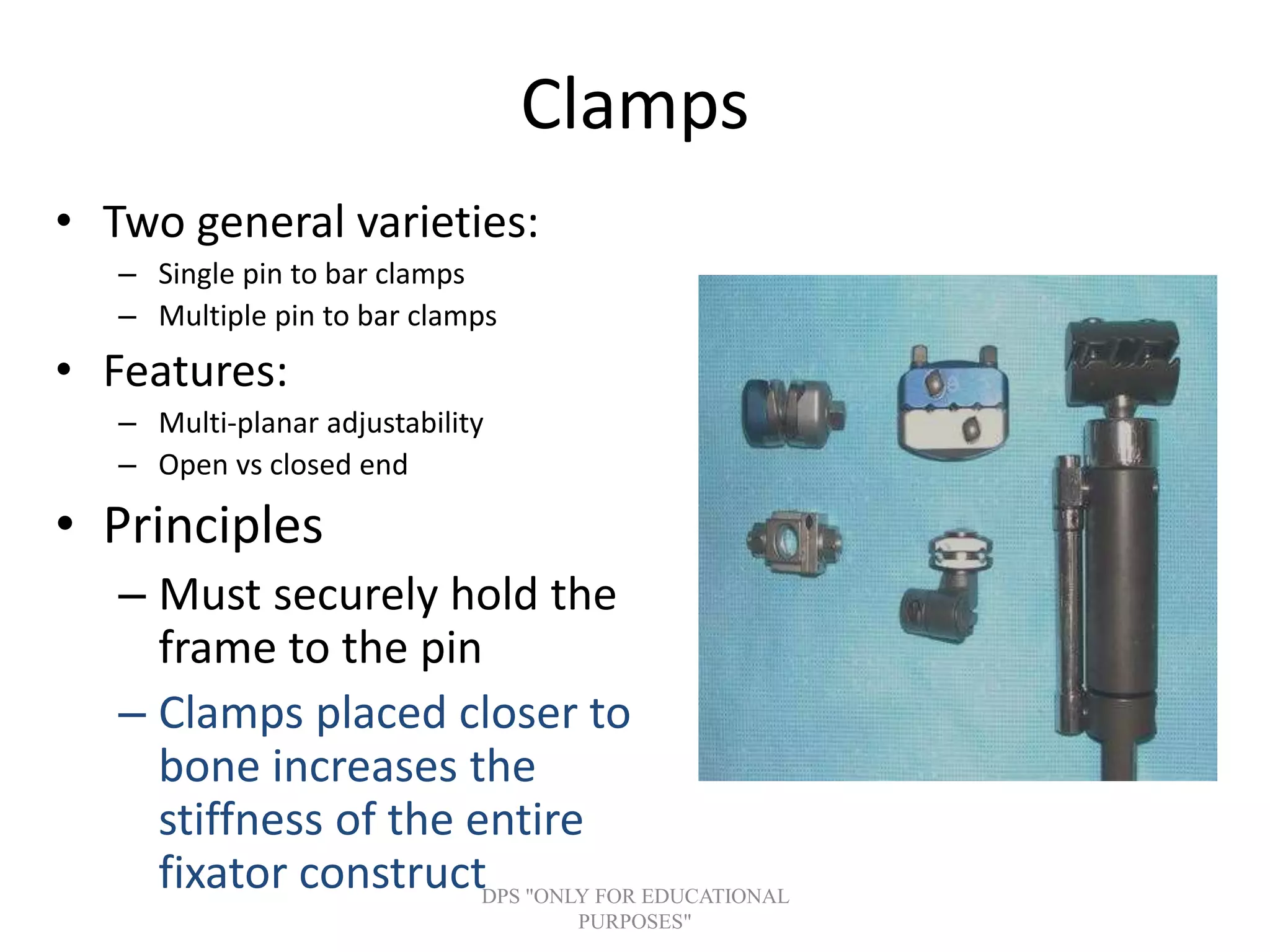
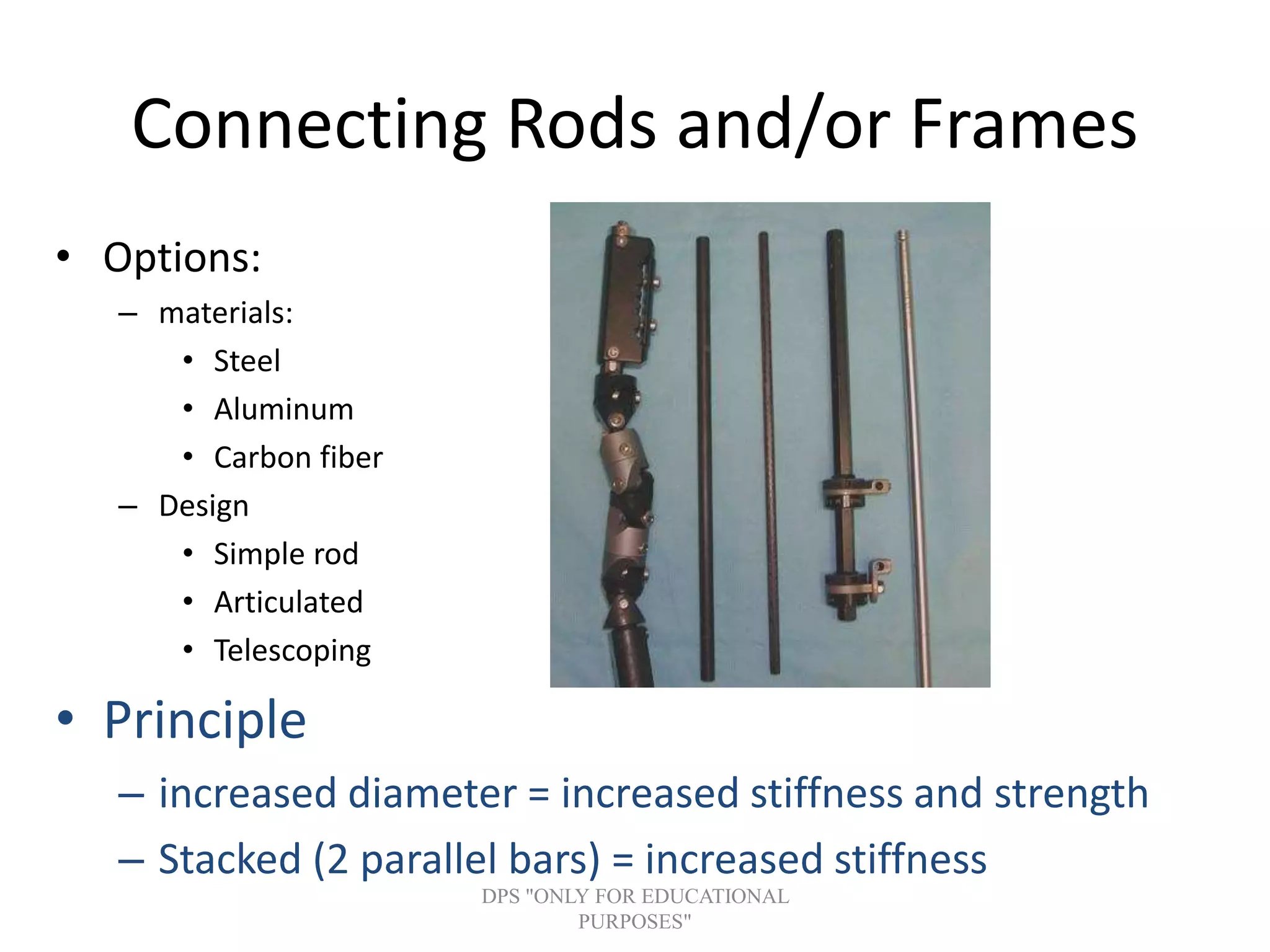
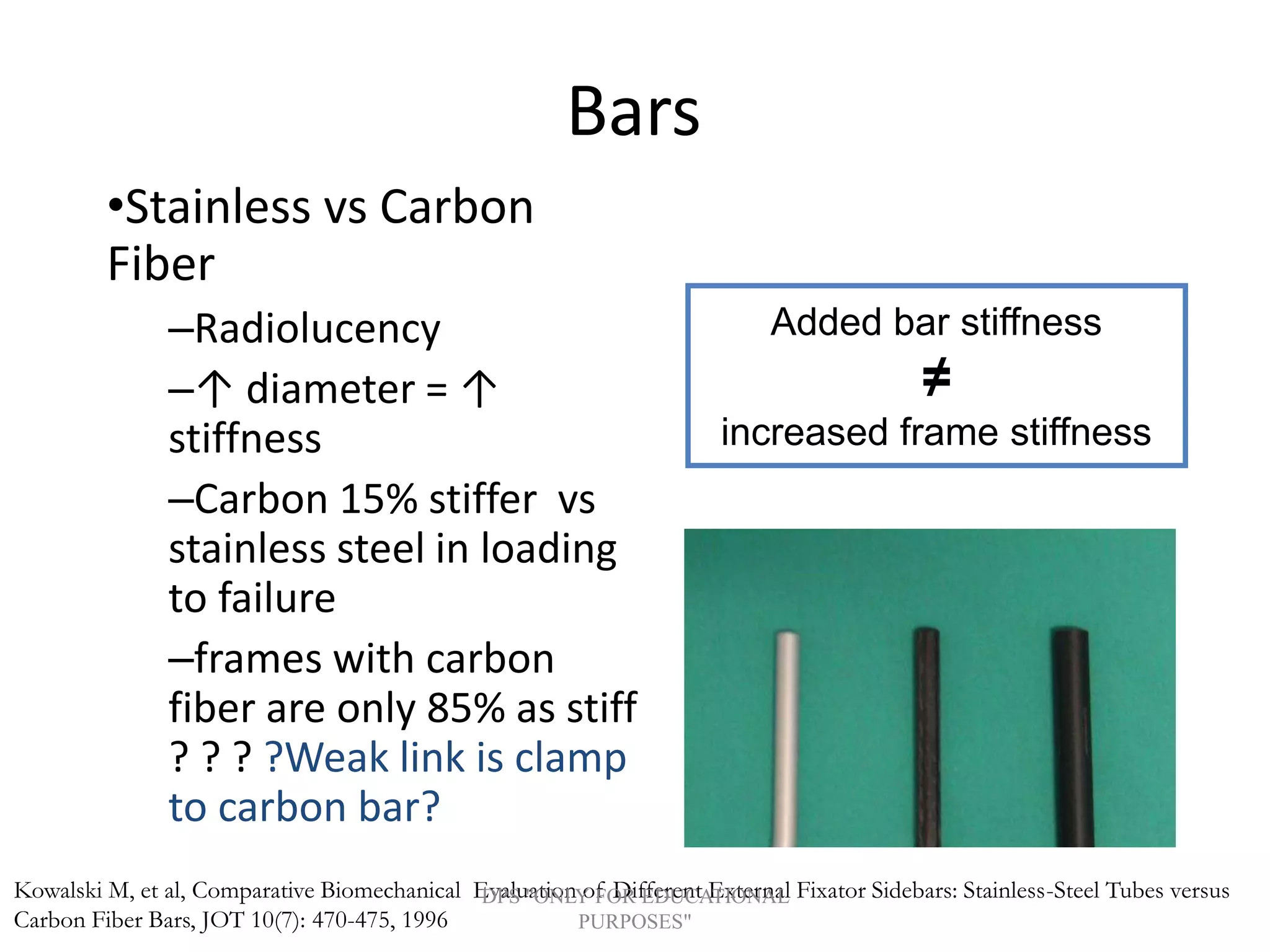
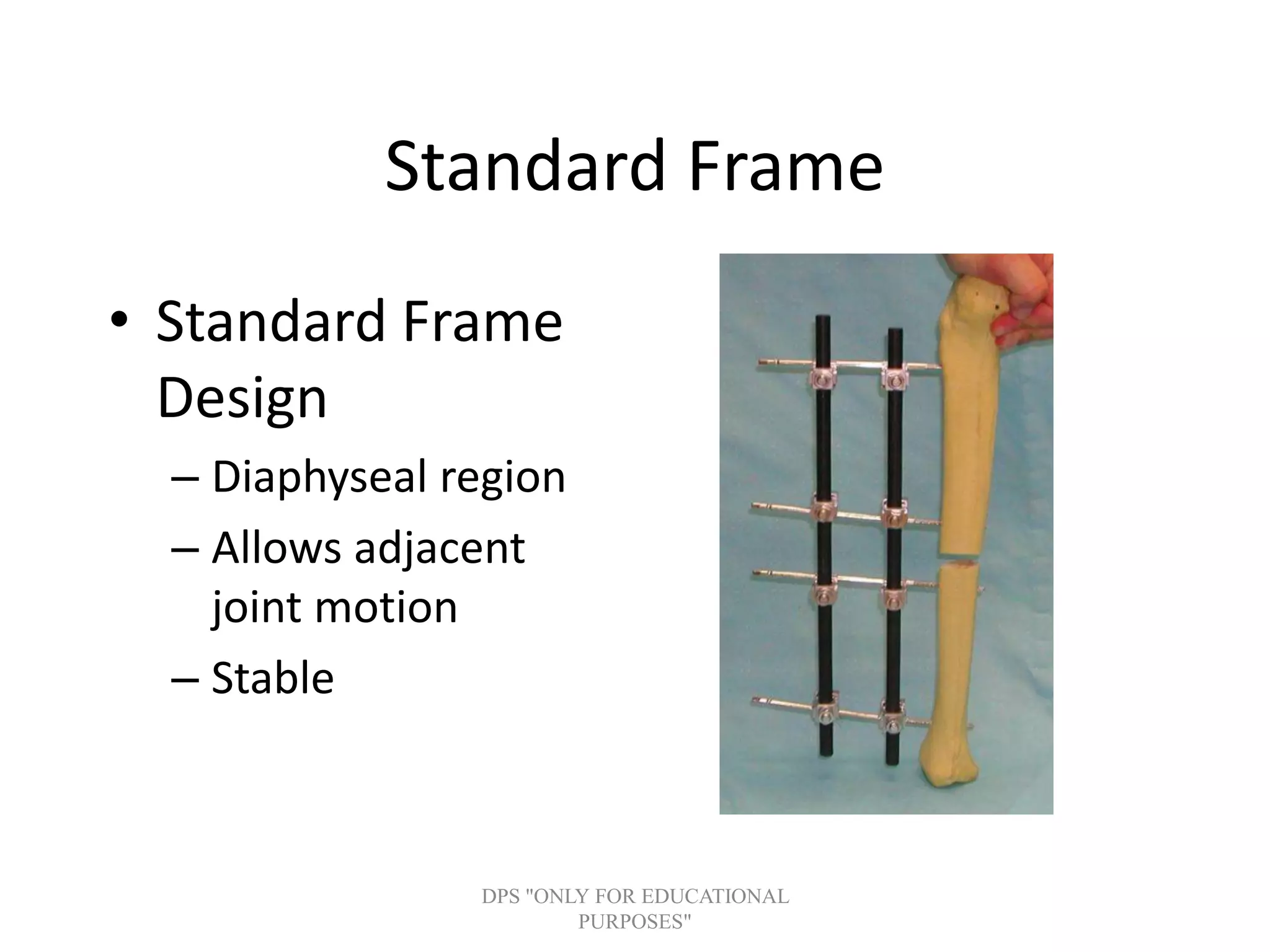
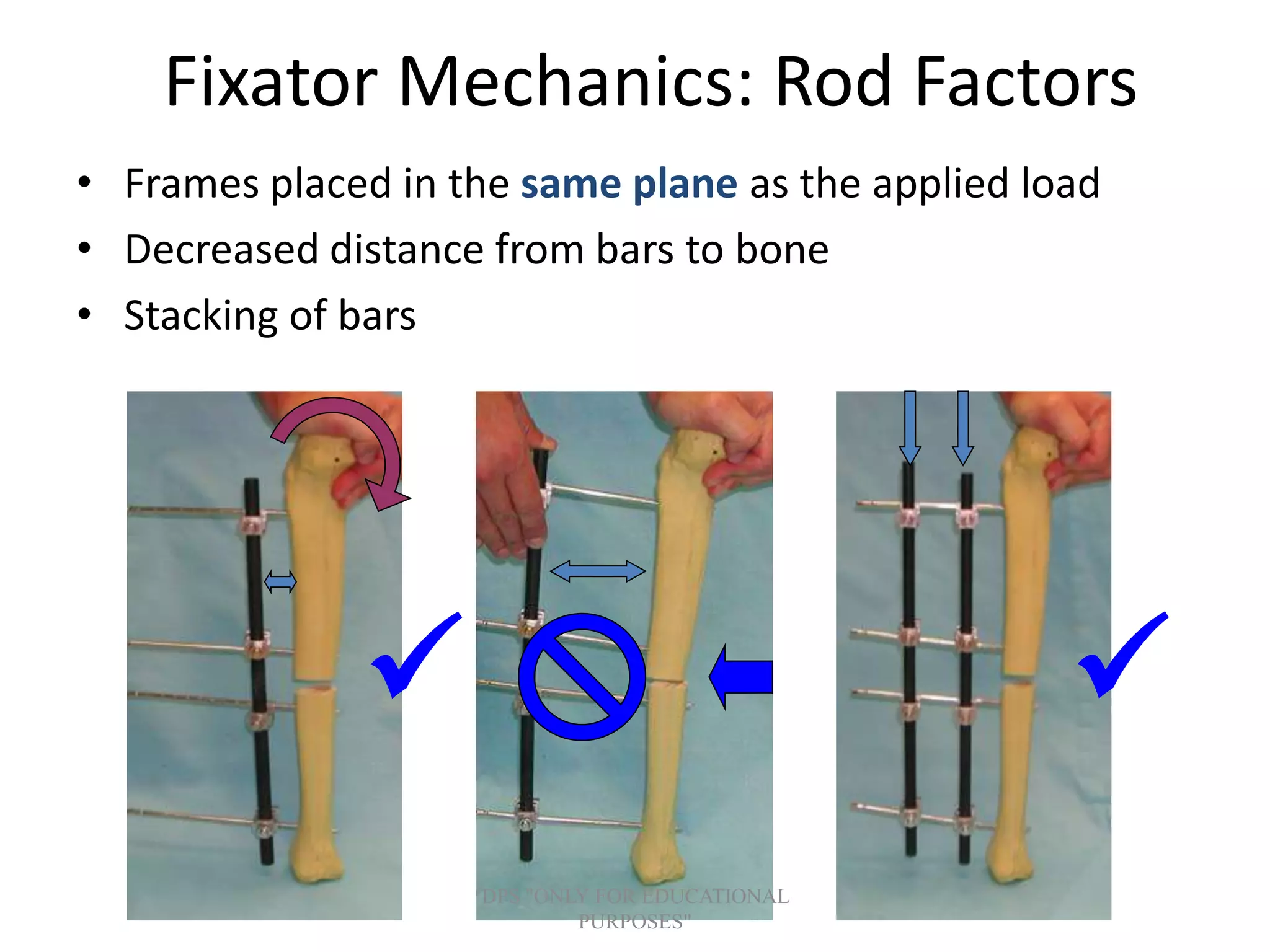
Types and features of clamps and rods used in external fixators, emphasizing adjustability and principles of frame stability.
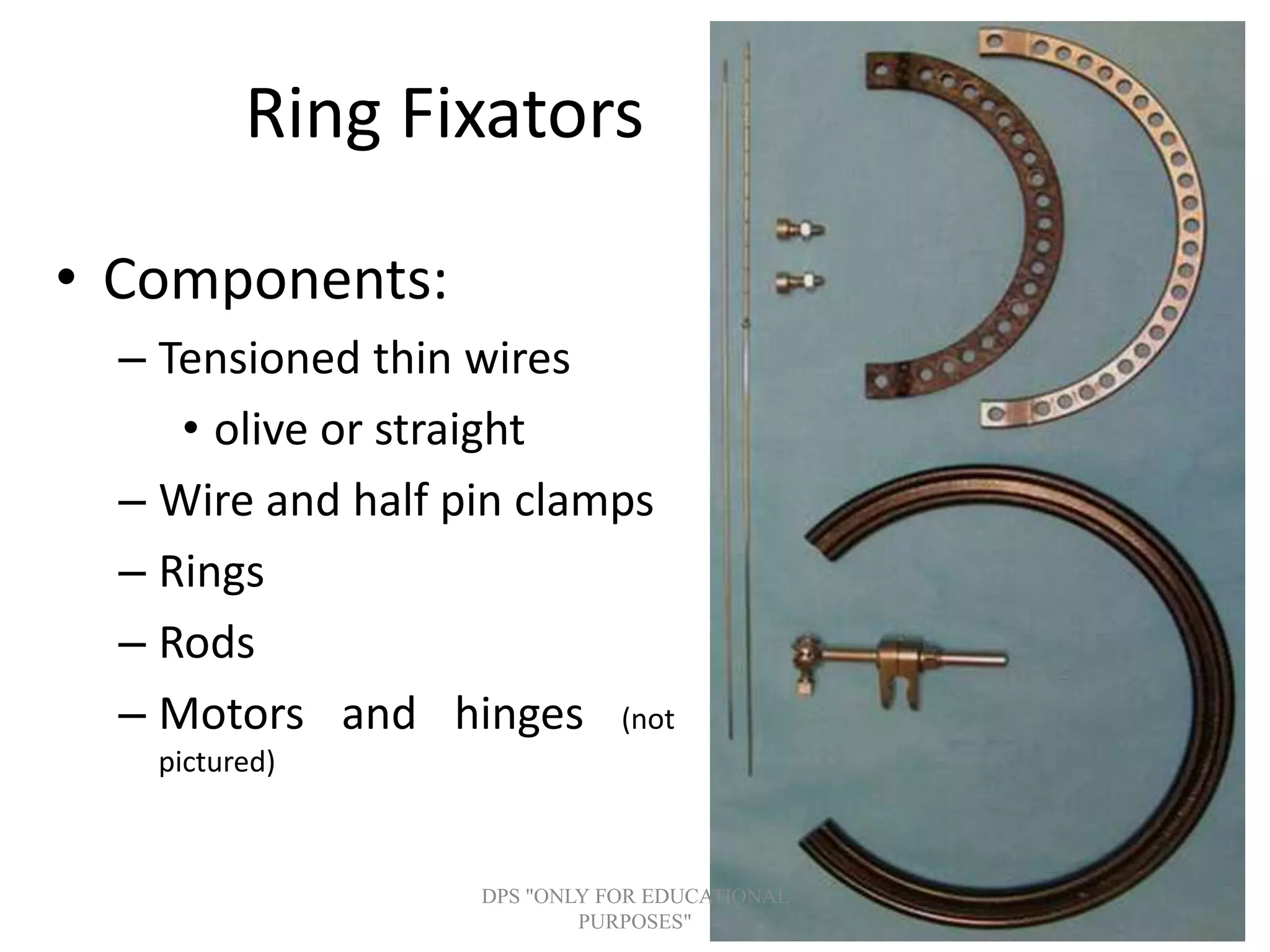
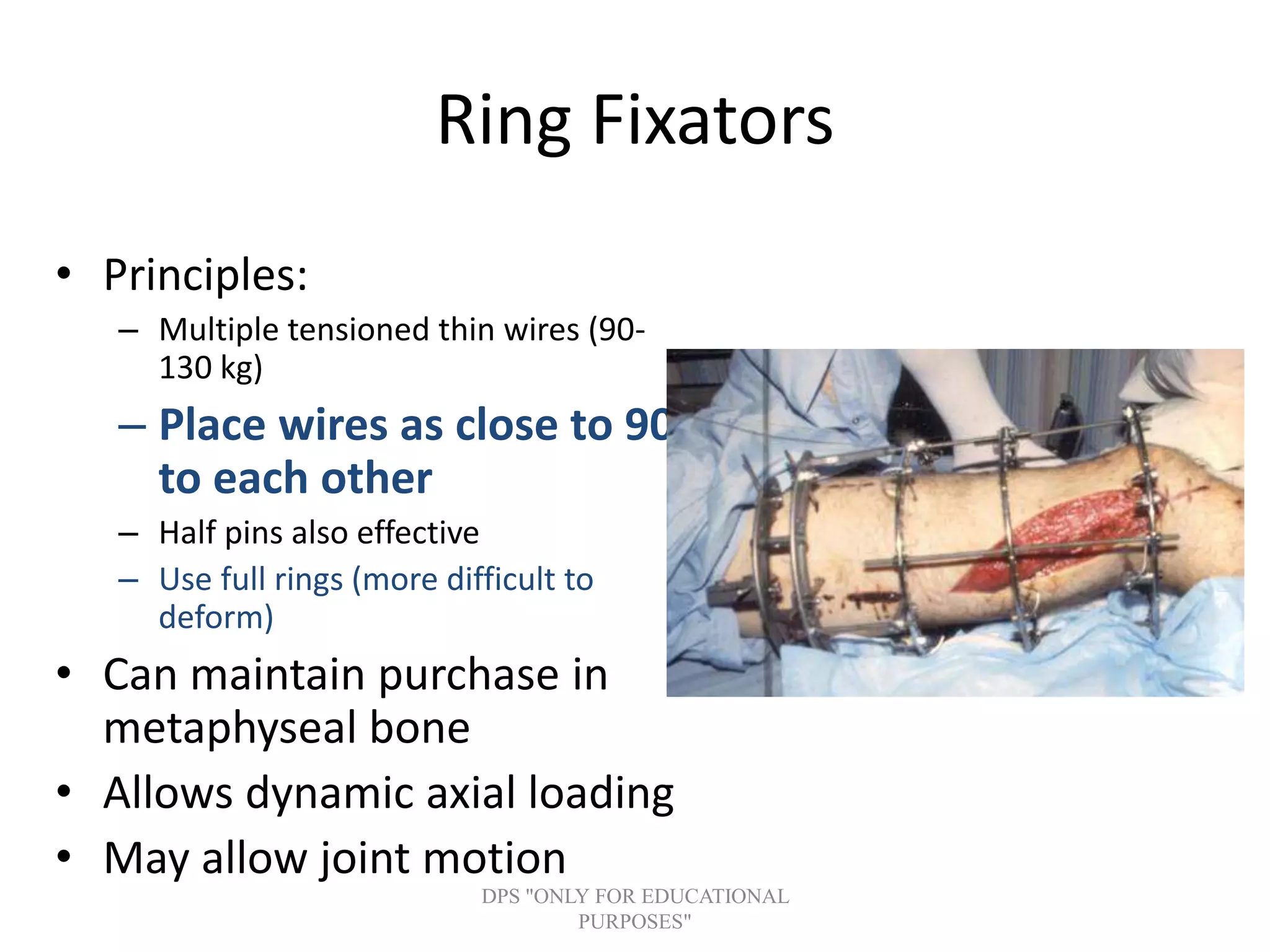
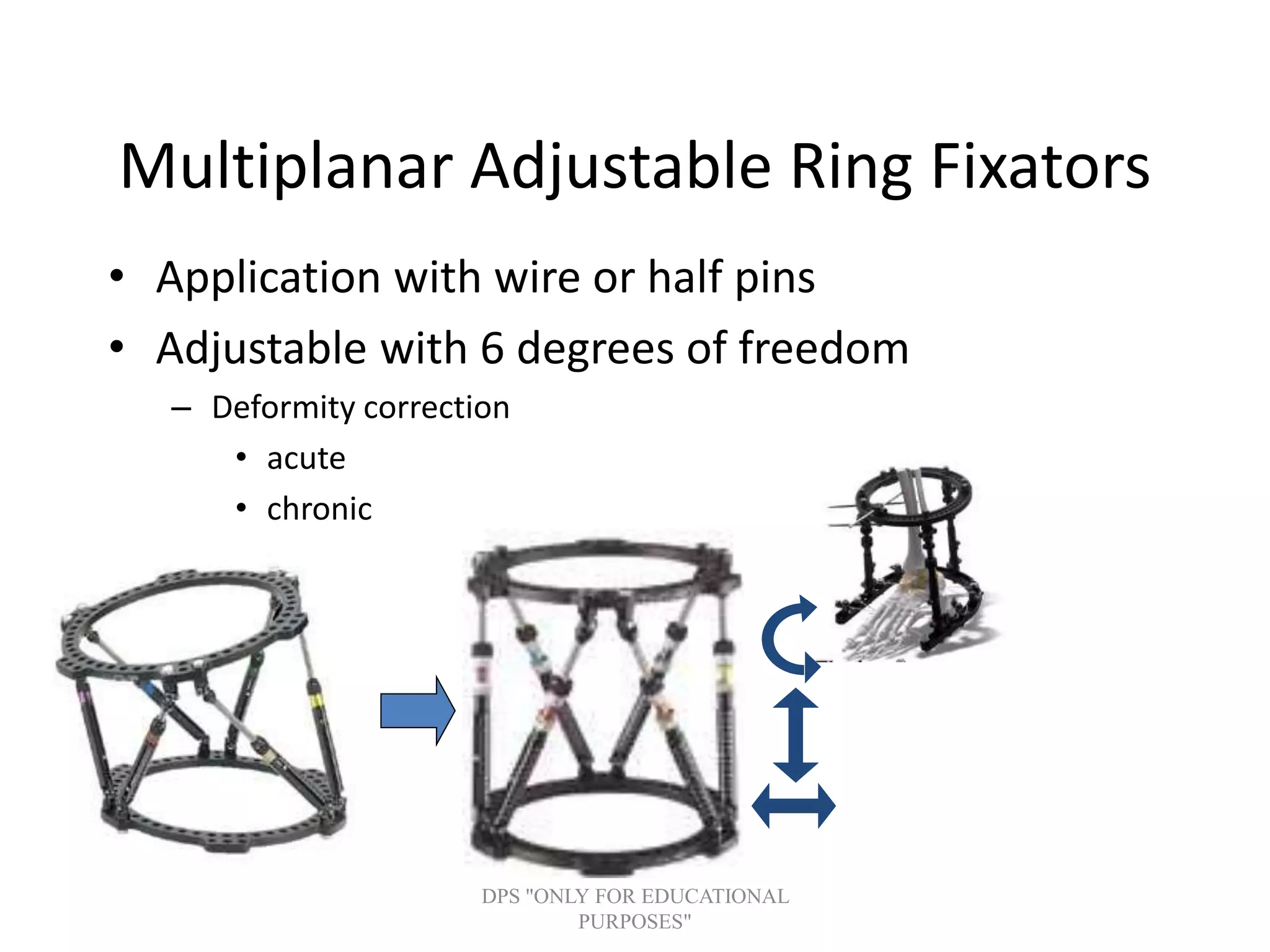
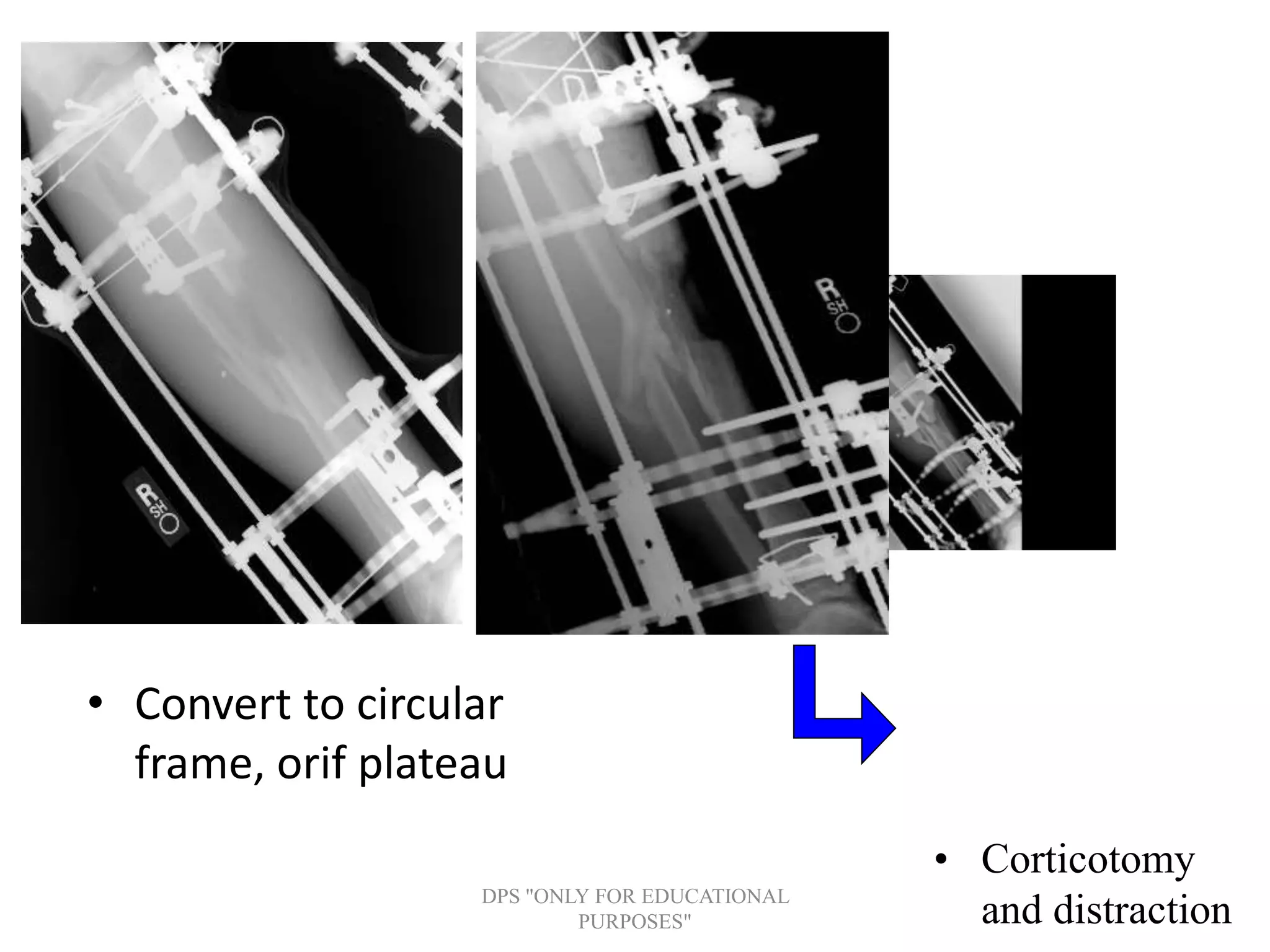
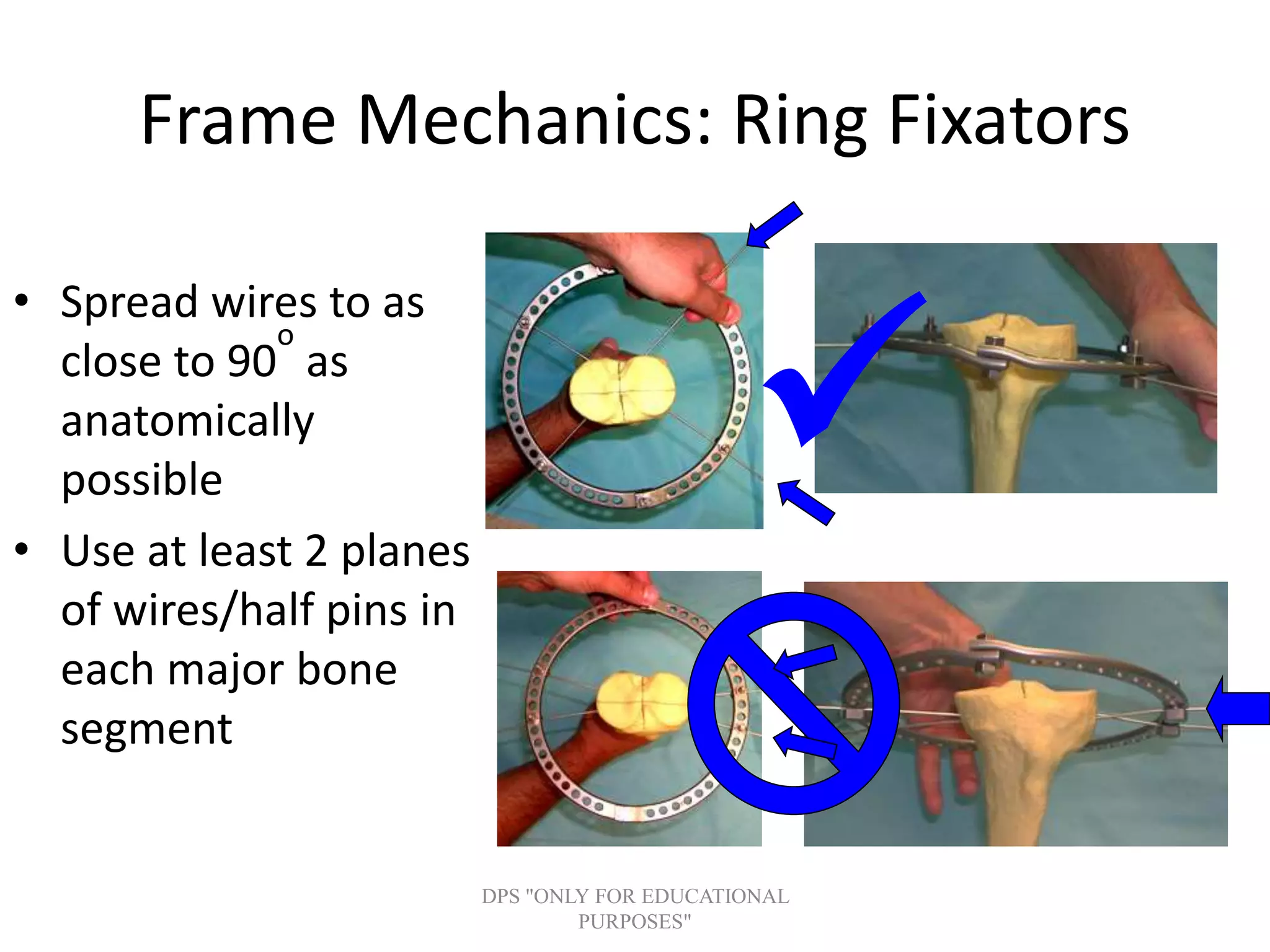
Components and principles of ring fixators, discussing tensioned wires and the ability to allow dynamic axial loading.
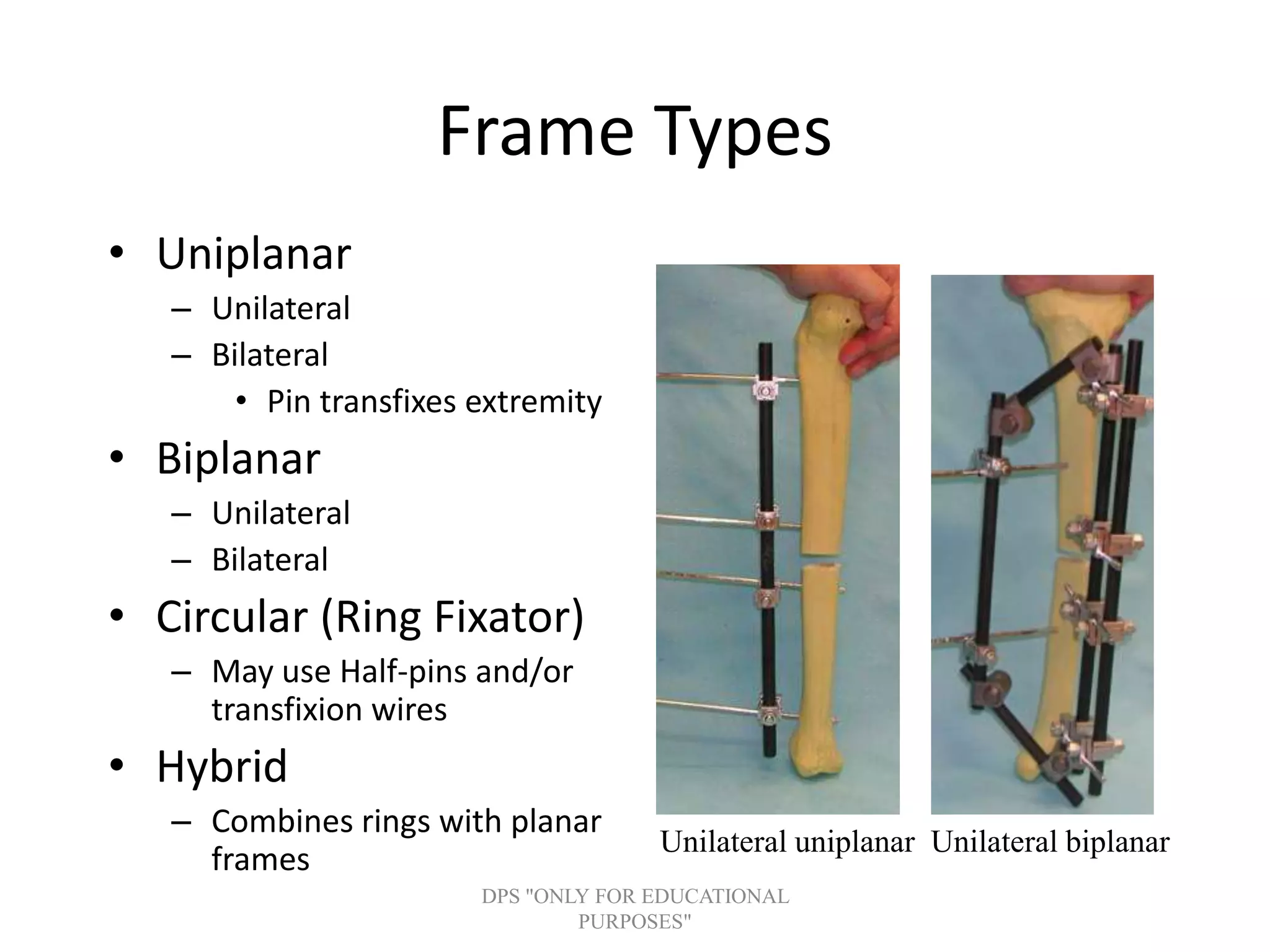
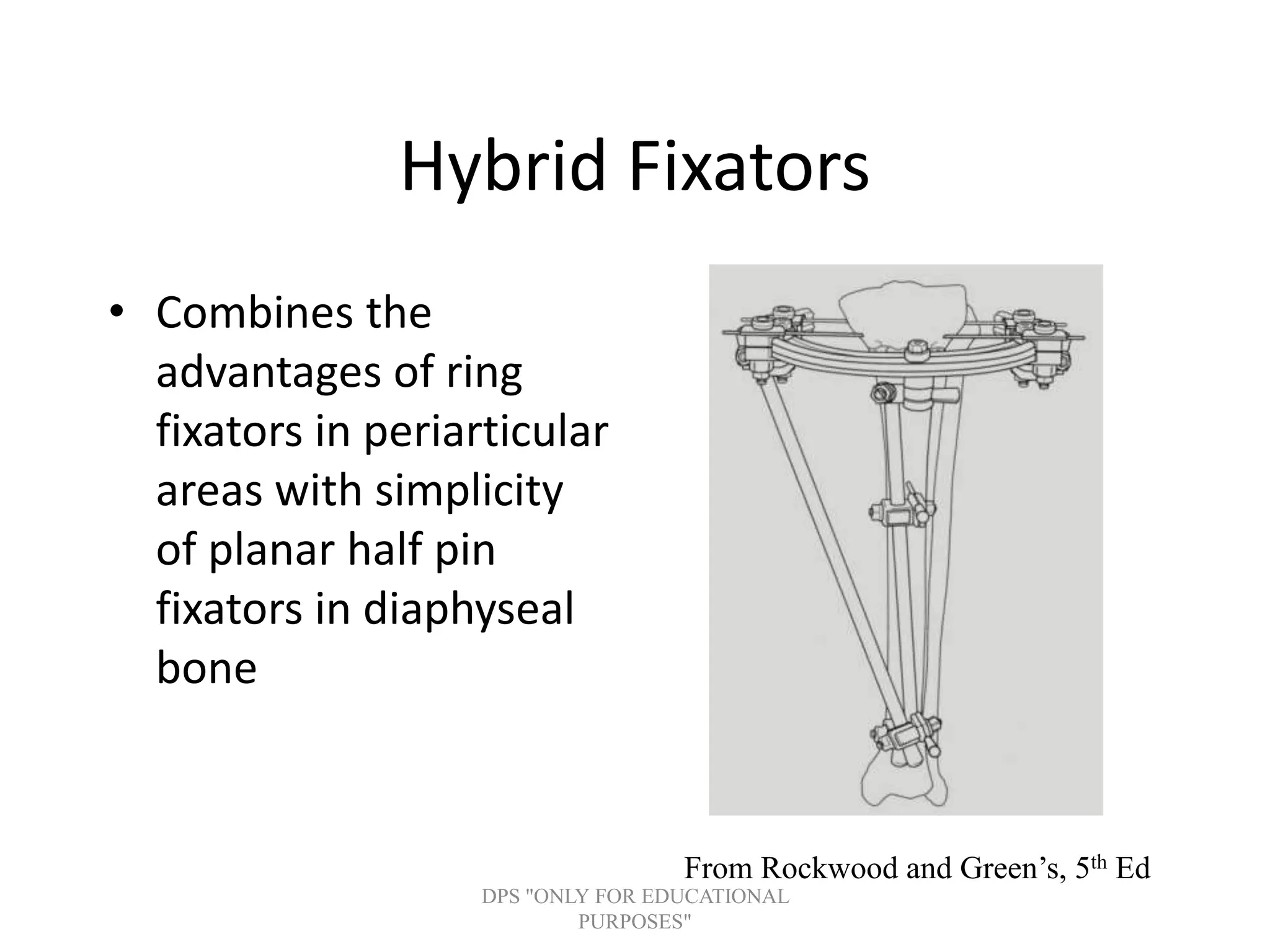
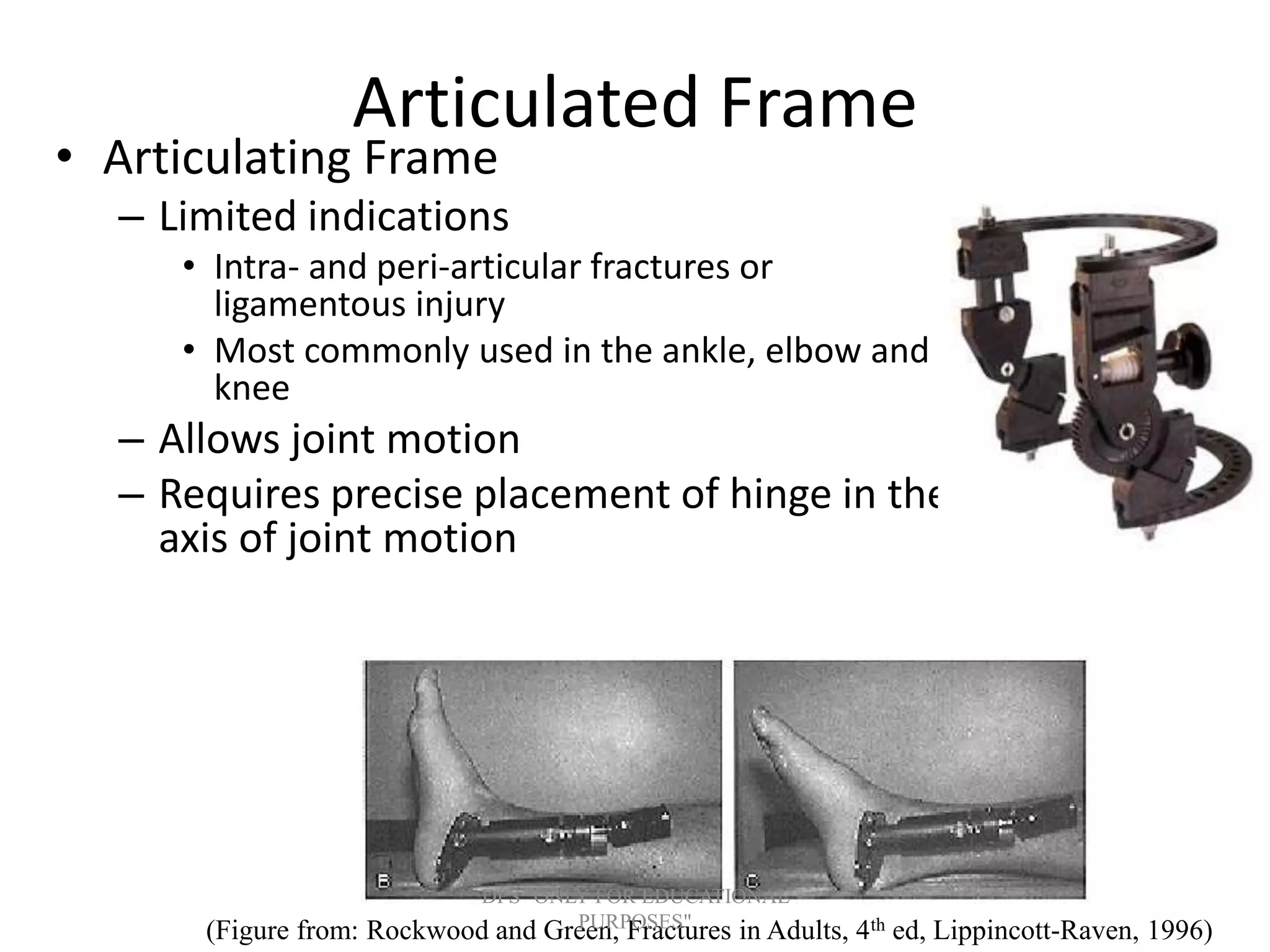
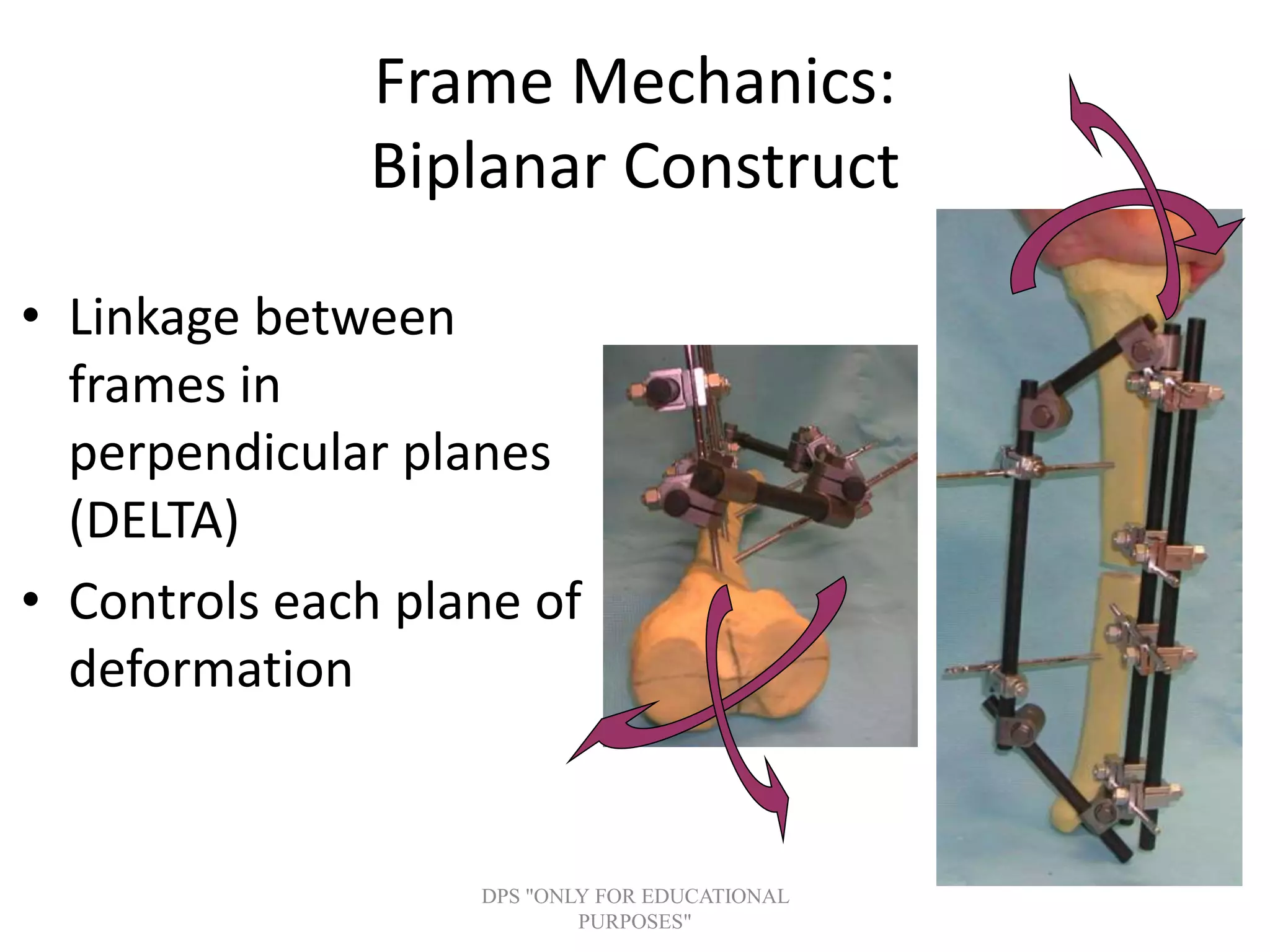
Explains various fixator frame types including uniplanar, biplanar, and hybrid options with indication details for applications in complex fractures. Biomechanics of external fixation, compatibility with MRI, and safe practices to enhance imaging and minimize risks.
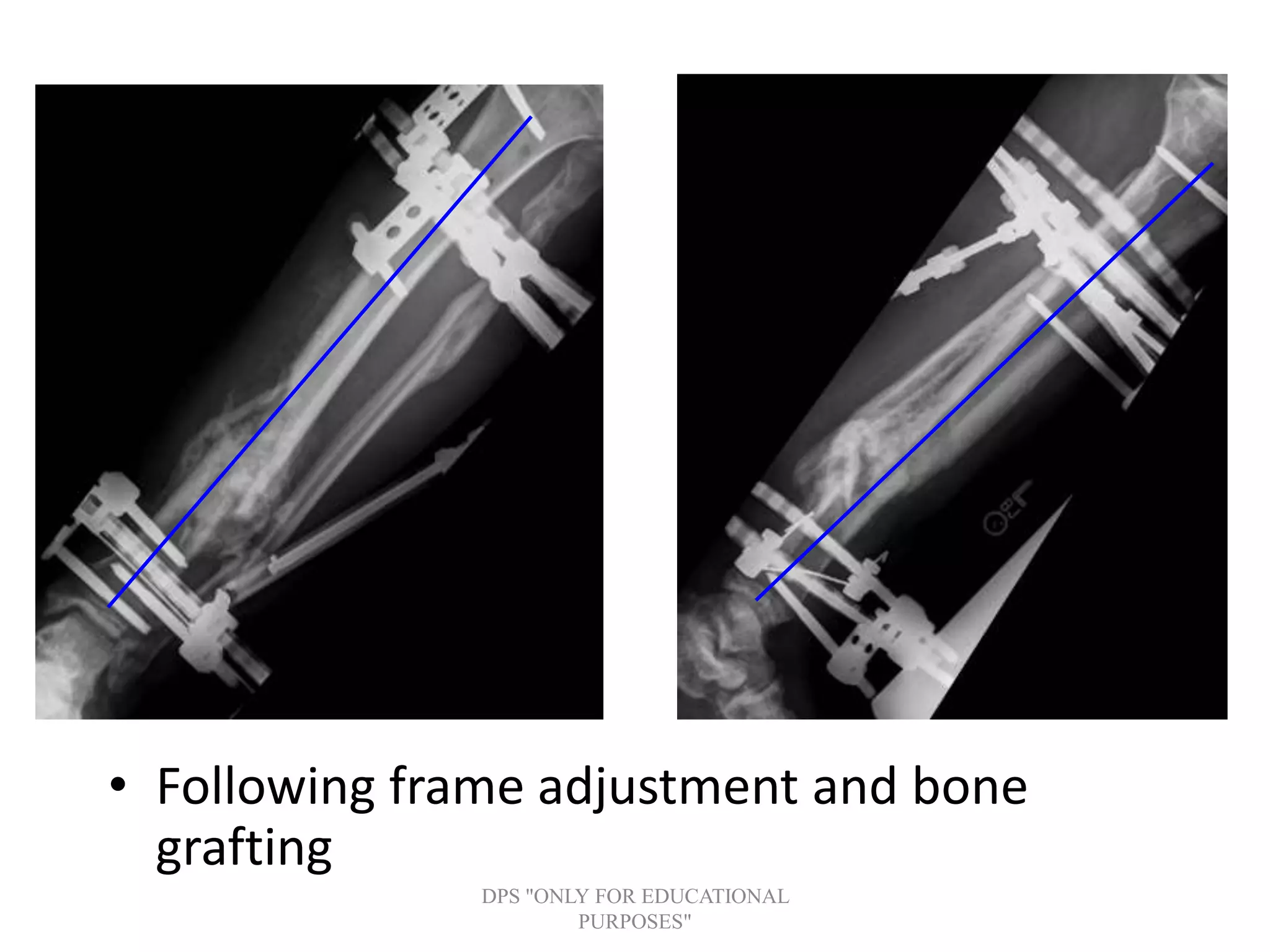
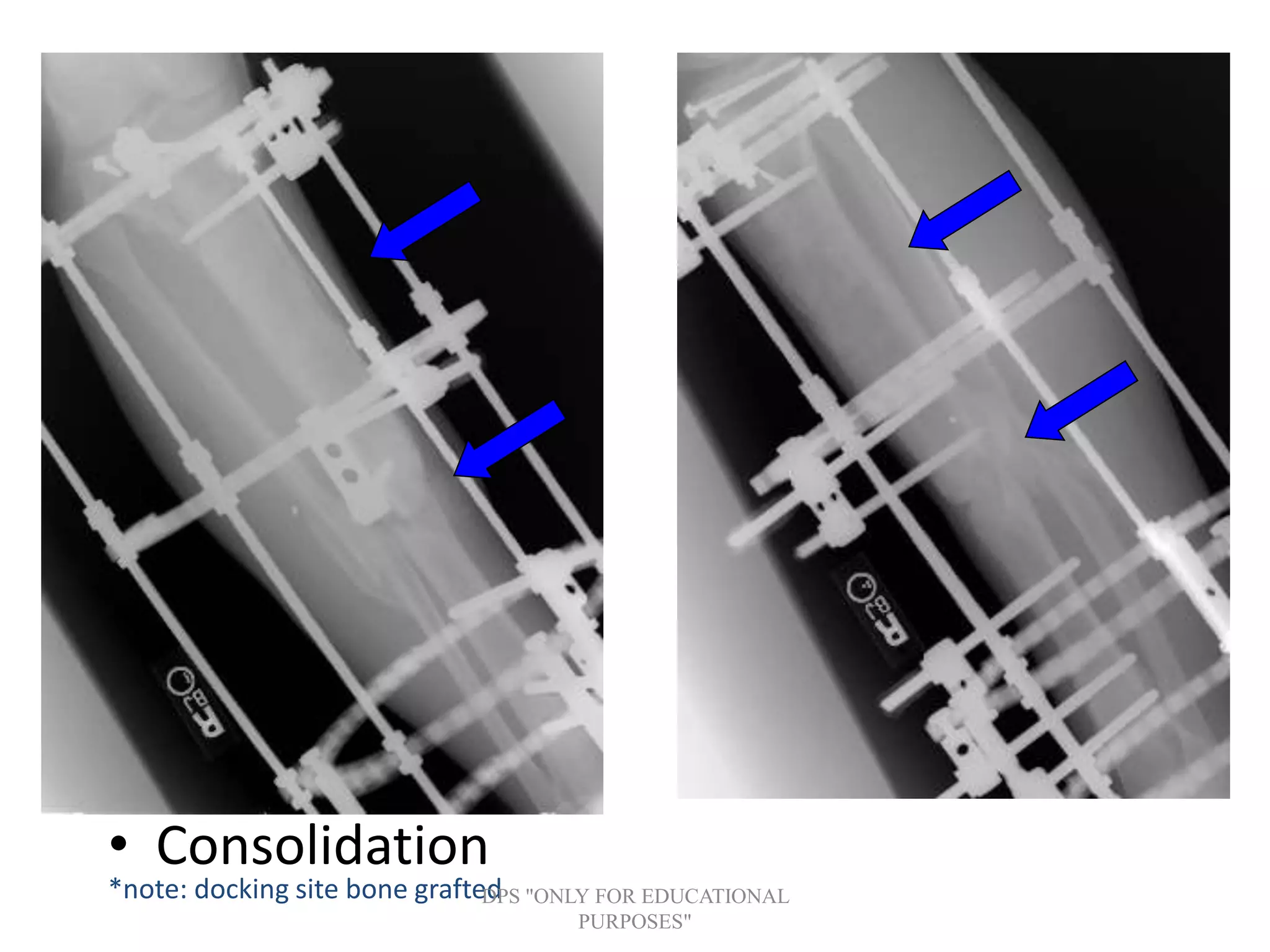
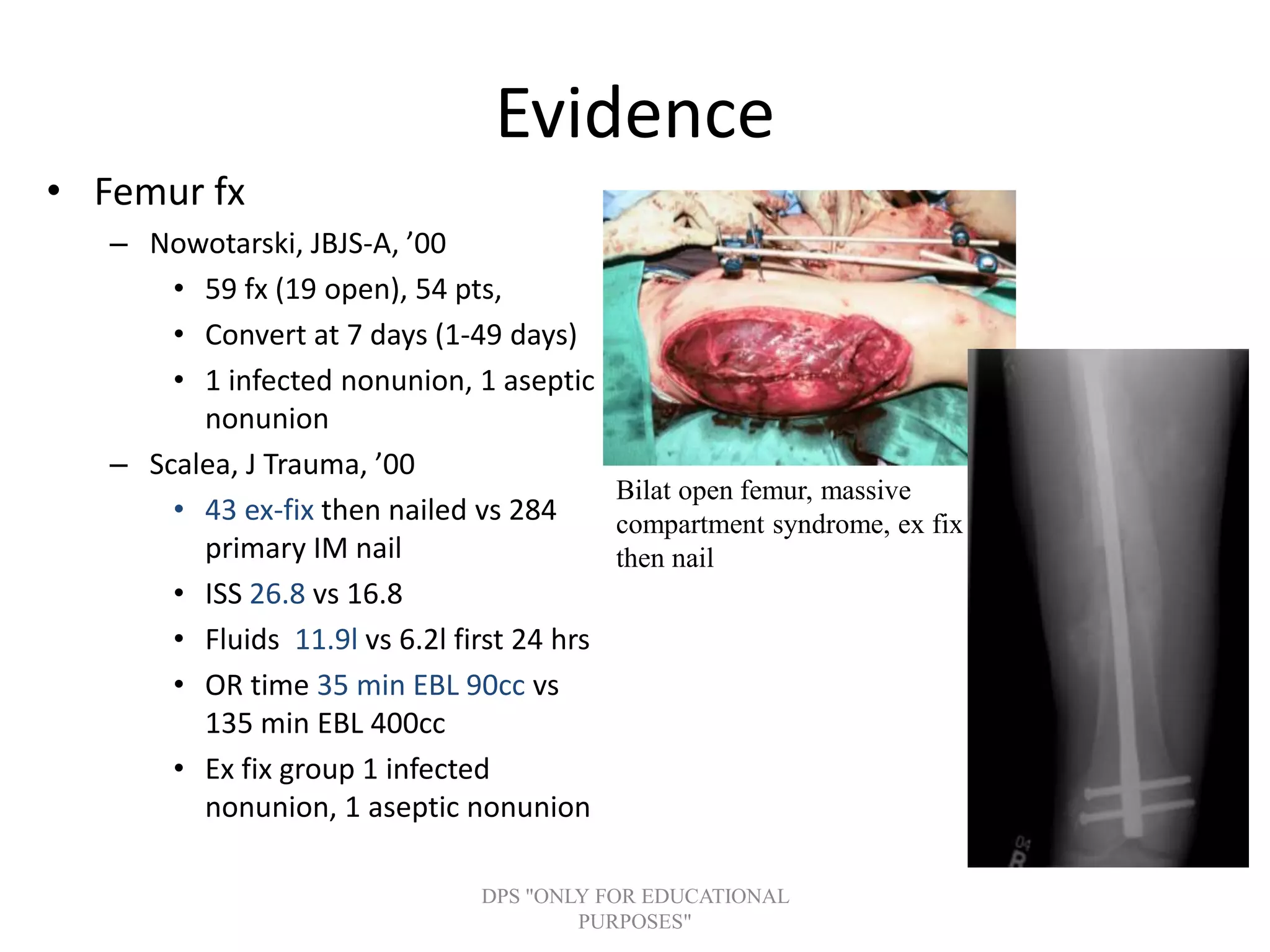
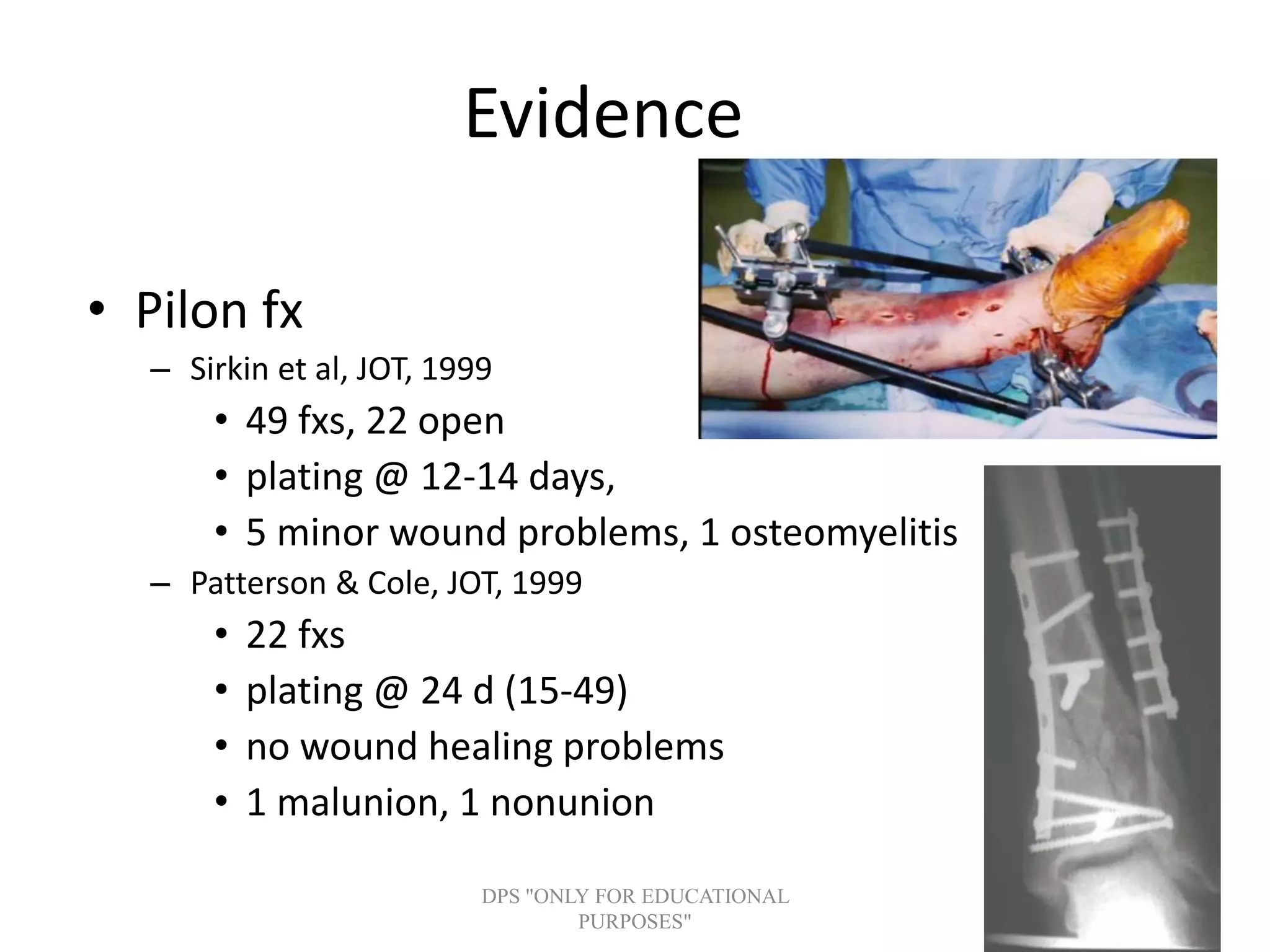
Details of advanced techniques for fracture management, including evidence from studies on efficacy and outcomes of conversion to internal fixation.
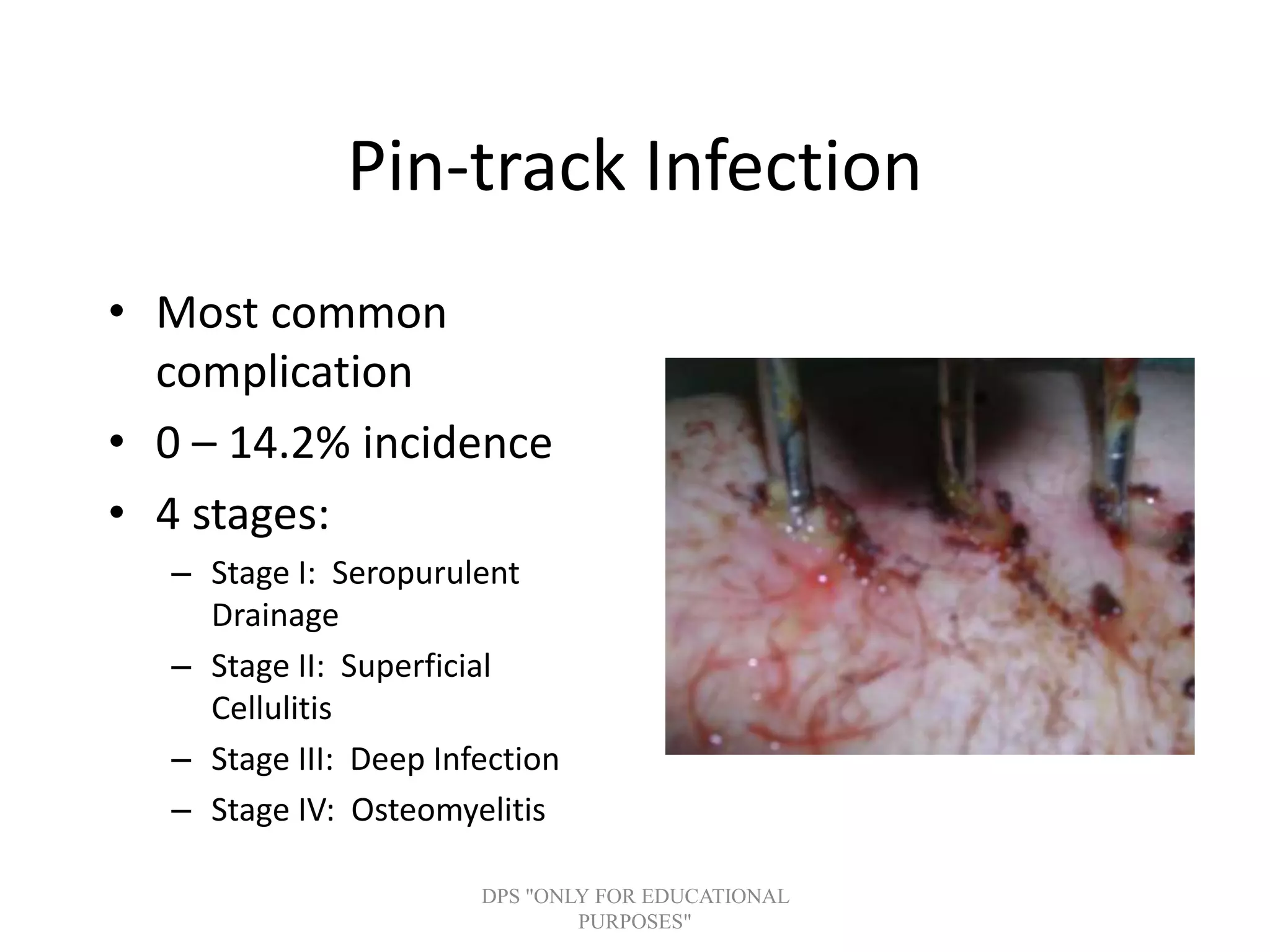
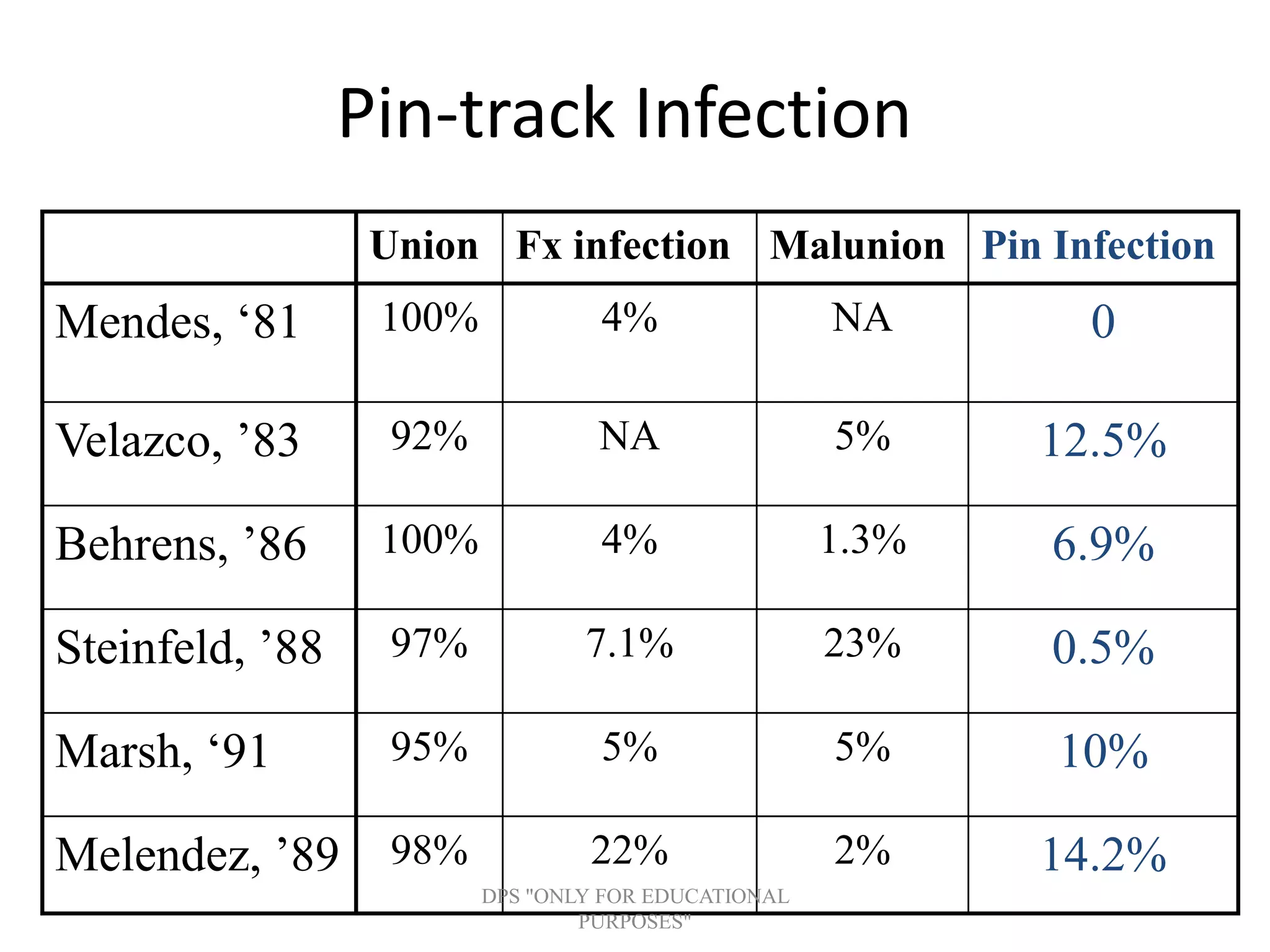
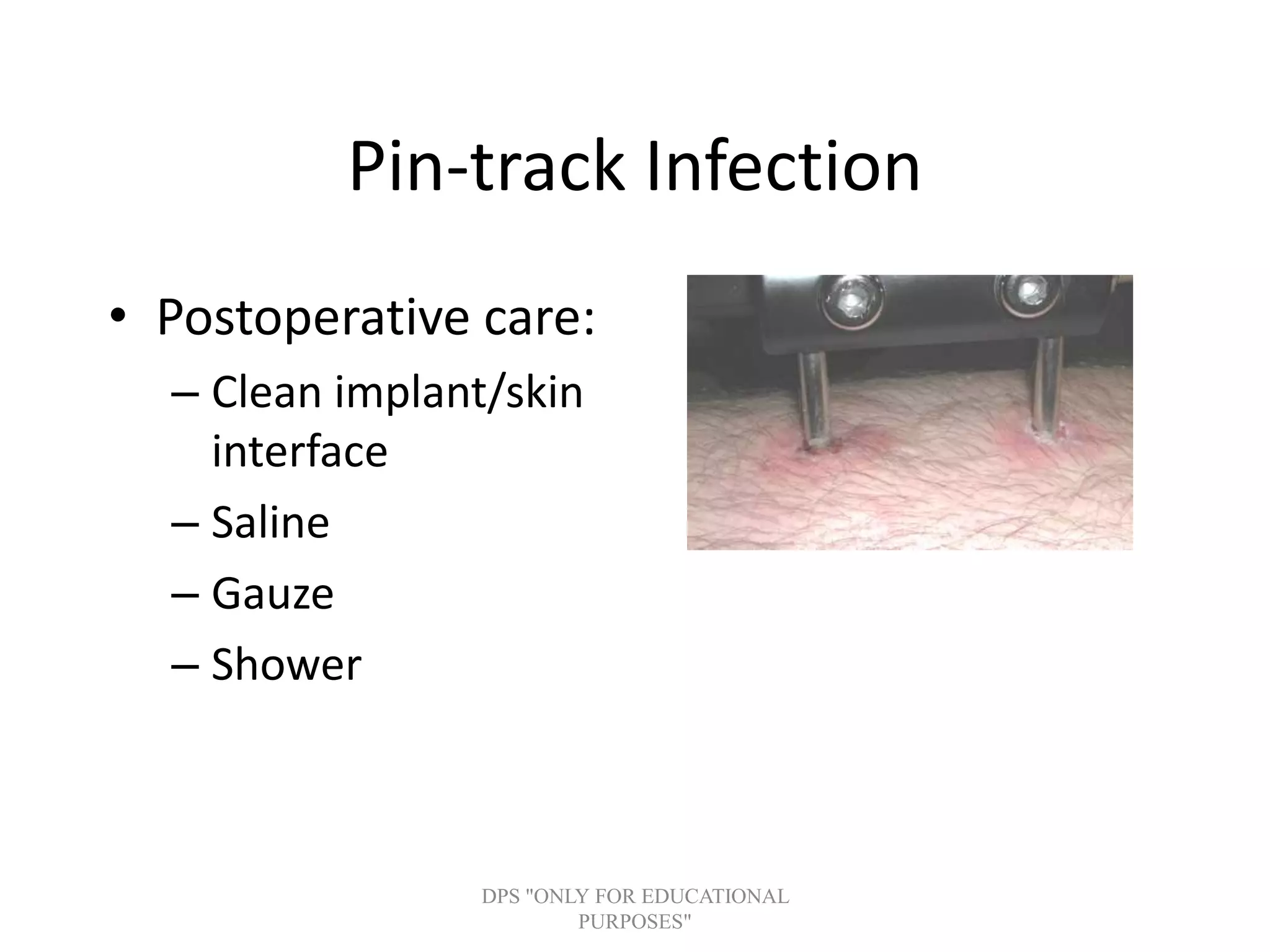
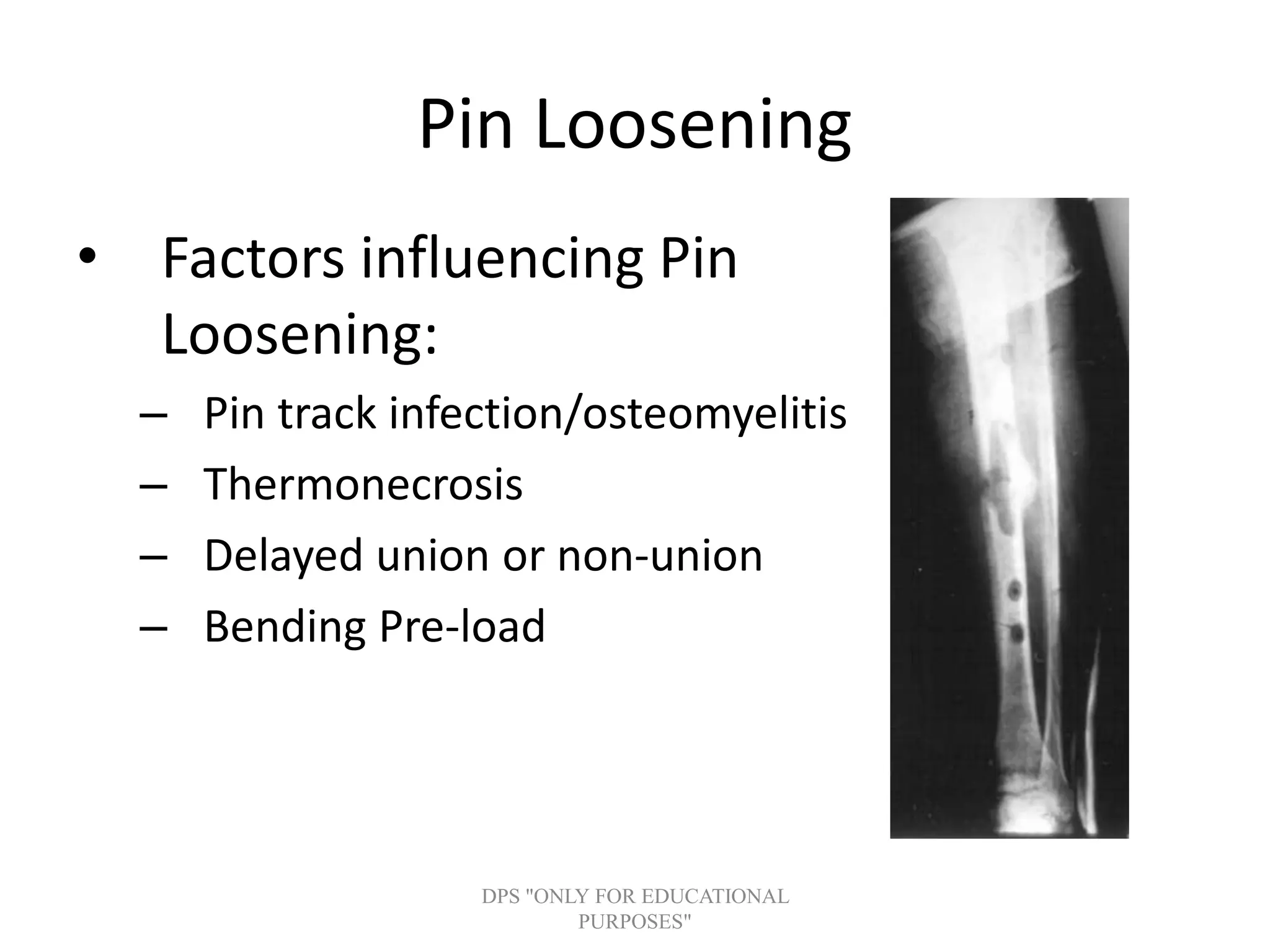
Discussion of common complications such as pin-track infections, malunion, non-union, and compartment syndrome with strategies for prevention and management.
Potential developments in pin technology, optimization for better healing, and construction tips for effective external fixation.