Downloaded 178 times










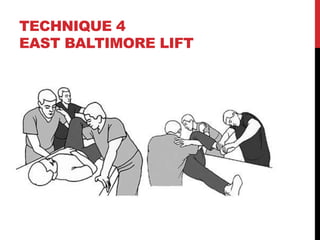

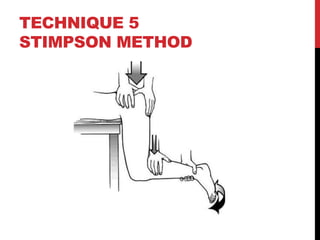





This document outlines techniques for reducing dislocated hips. It discusses various causes of hip dislocations including those from primary and revision total hip replacements, trauma, and hip resurfacing. Five techniques are described for reducing posterior hip dislocations: the Allis technique, Captain Morgan technique, Whistler technique, East Baltimore lift, and Stimpson method. Considerations for reduction include assessing other injuries, timing, and sedation. Post-reduction steps involve examining neurovascular status and imaging to check reduction. Complications can include nerve and artery injuries, fractures, and late issues like avascular necrosis.























































































