The document describes the anatomy and surgical procedures for lengthening the Achilles tendon. It discusses:
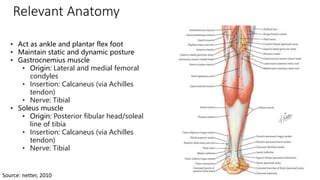
- The anatomy of the gastrocnemius and soleus muscles which connect to form the Achilles tendon
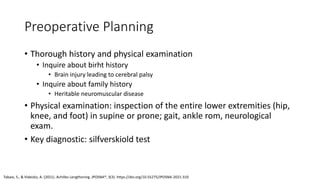
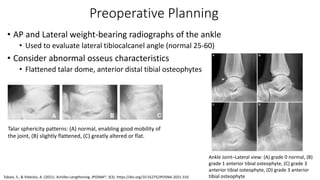
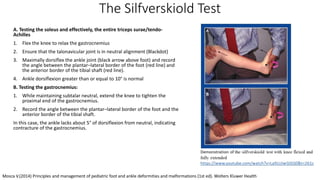
- Indications for Achilles tendon lengthening including contracture and limited ankle range of motion
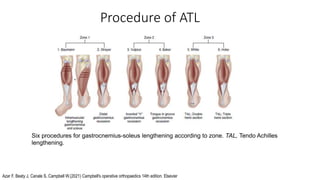
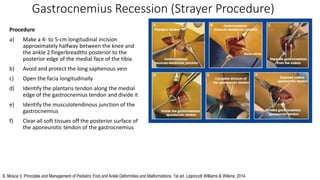
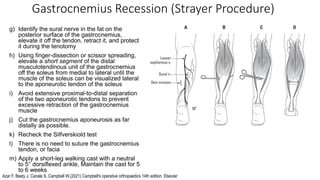
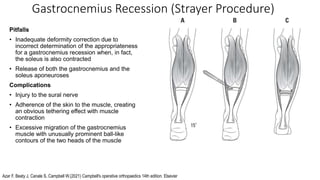
- Surgical techniques including gastrocnemius recession, intramuscular recession, and various Achilles tendon lengthening procedures
- Post-operative casting is typically used to maintain the correction
![References
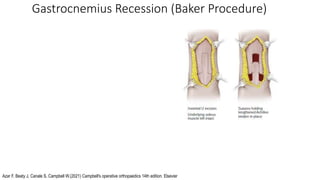
• Azar F, Beaty J, Canale S, Campbell W.(2021) Campbell's operative orthopaedics 14th edition. Elsevier
• S. Mosca V. Principles and Management of Pediatric Foot and Ankle Deformities and Malformations. 1st ed. Lippincott
Williams & Wilkins; 2014.
• Herring J. Tachdjian's pediatric orthopaedics From The Texas Scottish Rite Hospital For Children: Sixth Edition. 6th ed.
Elsevier; 2014.
• Weinstein S, Flynn J. Lovell and Winter's pediatric orthopaedics. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
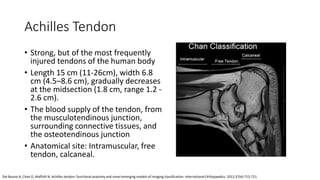
• Del Buono A, Chan O, Maffulli N. Achilles tendon: functional anatomy and novel emerging models of imaging classification.
International Orthopaedics. 2012;37(4):715-721.
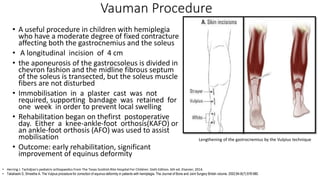
• Tabaie S, Videckis A. Achilles Lengthening. jposna [Internet]. 2021Jul.26 [cited 2022Jul.15];3(3). Available from:
https://www.jposna.org/ojs/index.php/jposna/article/view/310
• Rong K, Li X, Ge W, Xu Y, Xu X. Comparison of the efficacy of three isolated gastrocnemius recession procedures in a
cadaveric model of gastrocnemius tightness. International Orthopaedics. 2015;40(2):417-423.
• Firth G, McMullan M, Chin T, Ma F, Selber P, Eizenberg N et al. Lengthening of the Gastrocnemius-Soleus Complex. 2022.
• Volpon J, Natale L. Critical evaluation of the surgical techniques to correct the equinus deformity. Revista do Colégio
Brasileiro de Cirurgiões. 2019;46(1).
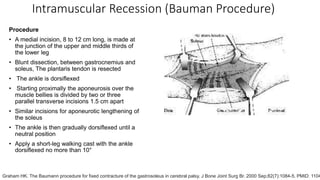
• Graham HK. The Baumann procedure for fixed contracture of the gastrosoleus in cerebral palsy. J Bone Joint Surg Br. 2000
Sep;82(7):1084-5. PMID: 11041608.](https://image.slidesharecdn.com/achillestendonlengthening-230109042601-a47a67ed/85/Achilles-Tendon-Lengthening-pptx-26-320.jpg)



































































