Downloaded 123 times
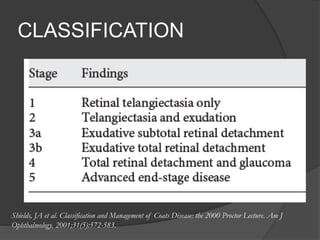
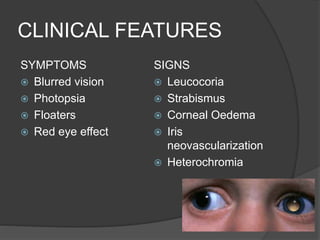
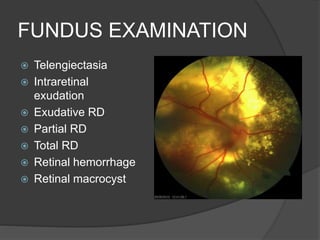

This document discusses Coats' disease, a rare eye condition characterized by abnormal blood vessels in the retina. It presents in children, more often in boys than girls, and causes vision loss. Symptoms include blurred vision and eye swelling. Examination shows leaking blood vessels, fluid buildup, and retinal detachment. Treatment depends on the stage, ranging from close monitoring to laser therapy, cryotherapy, surgery, and in severe cases, eye removal. The goal is to preserve vision or the eye's structure.




























































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)














