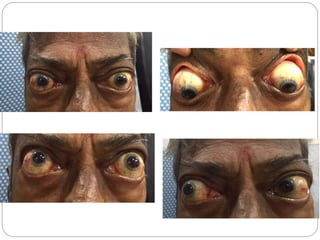
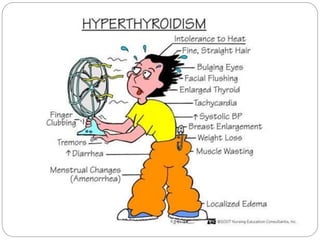
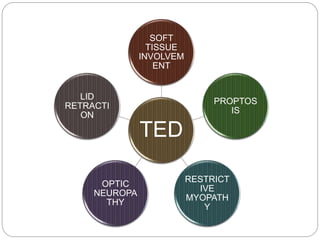
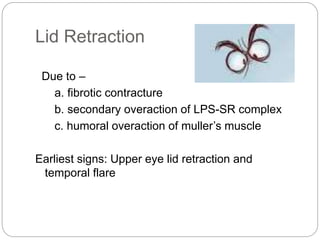
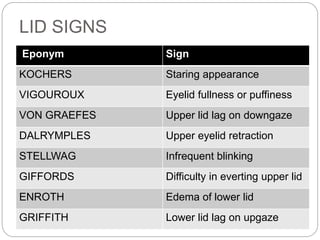
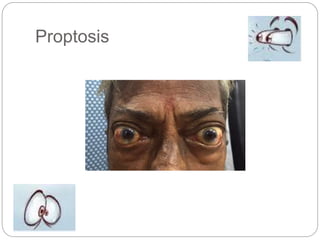
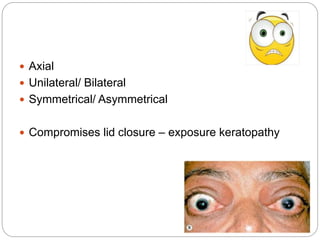
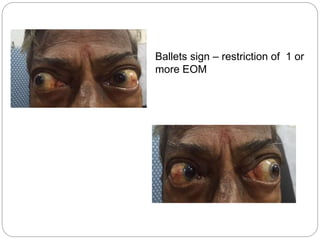
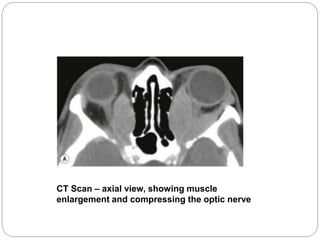
This document presents a case study of a 67-year-old male with thyroid eye disease. On examination, he was found to have proptosis, lid retraction, and restriction of eye movement in the left eye. Imaging showed compression of the optic nerve. The patient has a history of thyroid disease treated with oral medications. Thyroid eye disease is described as having two stages - an inflammatory stage and a fibrotic stage. The document outlines the key signs and symptoms of thyroid eye disease including soft tissue involvement, proptosis, restrictive myopathy, optic neuropathy, and lid retraction. The conclusion emphasizes treating each manifestation individually while considering the overall disease.