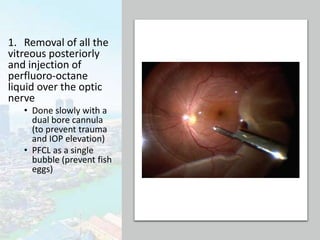
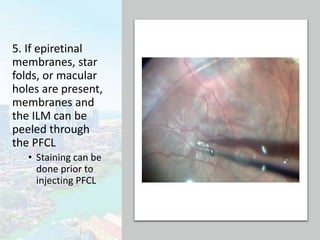
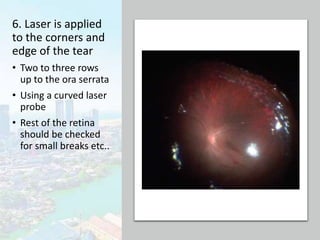
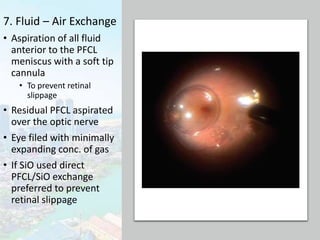
This document discusses giant retinal tears (GRTs), which are full thickness circumferential retinal tears of more than 900 of the retina. GRTs are often associated with vitreous detachment and can occur spontaneously or due to conditions like high myopia. The main management approaches are vitrectomy using perfluorocarbon liquids, sometimes combined with laser photocoagulation or scleral buckling. Vitrectomy involves removing the vitreous gel, unfolding the retina using perfluorocarbon liquids, applying laser to the tear edges, and exchanging the liquids for gas or silicone oil. The reattachment rate after surgery is 80-90% with a final rate of 94-100%, though visual outcomes are often poor if prolif



![PATHOGENESIS
• Liquefaction of central vitreous
• Peripheral vitreous condensation
• Concomitant traction at the vitreous base
• The neurosensory retina tears circumferentially in
the area of the posterior vitreous base
• Vitreous gel attached to the anterior flap
• Posterior flap moves freely and can fold upon itself
[In retinal dialyses the vitreous is adherent to the
posterior aspect of the retinal tear, therefore the
retina is not very mobile – laser/ scleral buckle]](https://image.slidesharecdn.com/giantretinaltears-210203134836/85/Giant-Retinal-Tears-5-320.jpg)