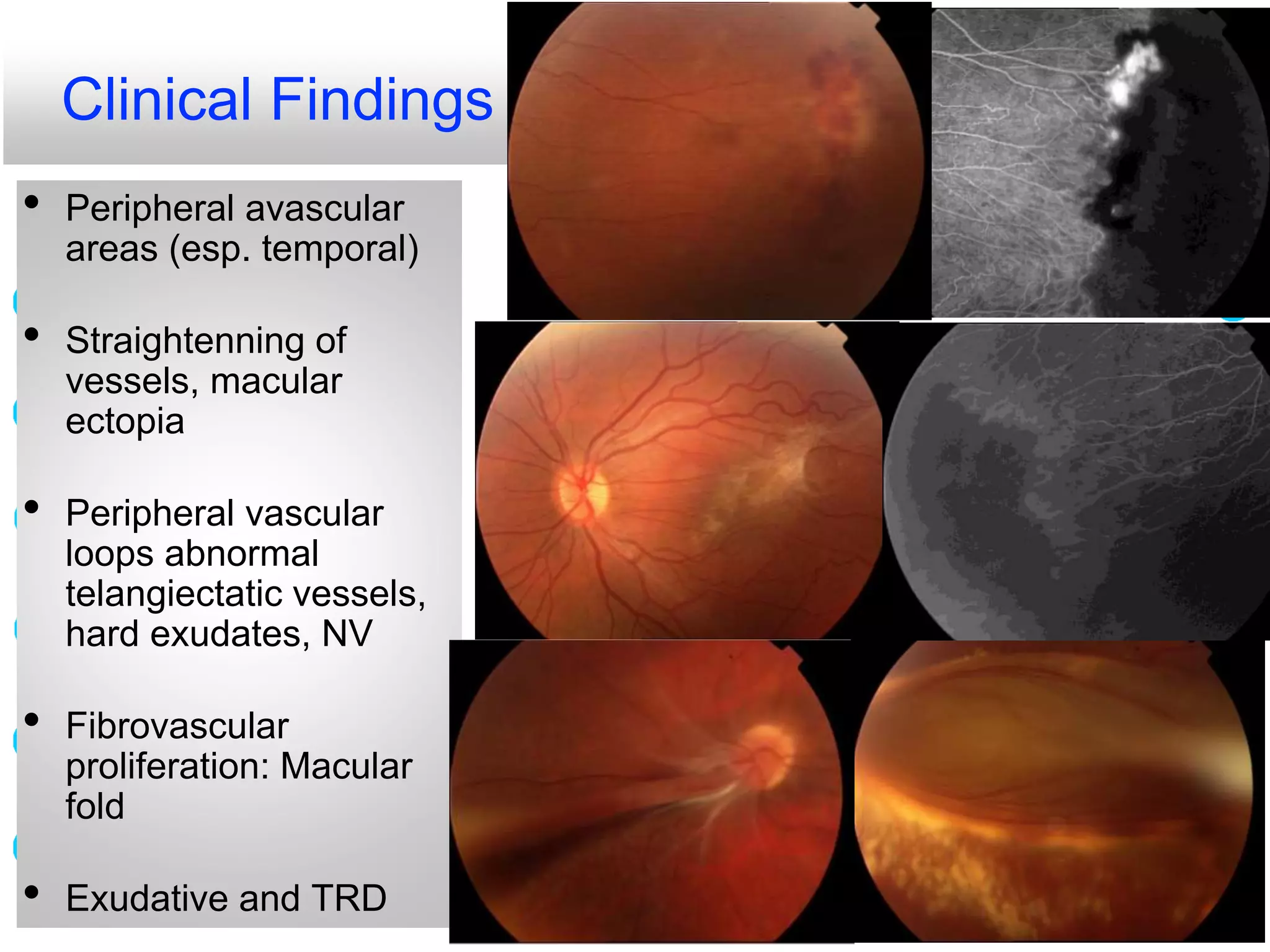
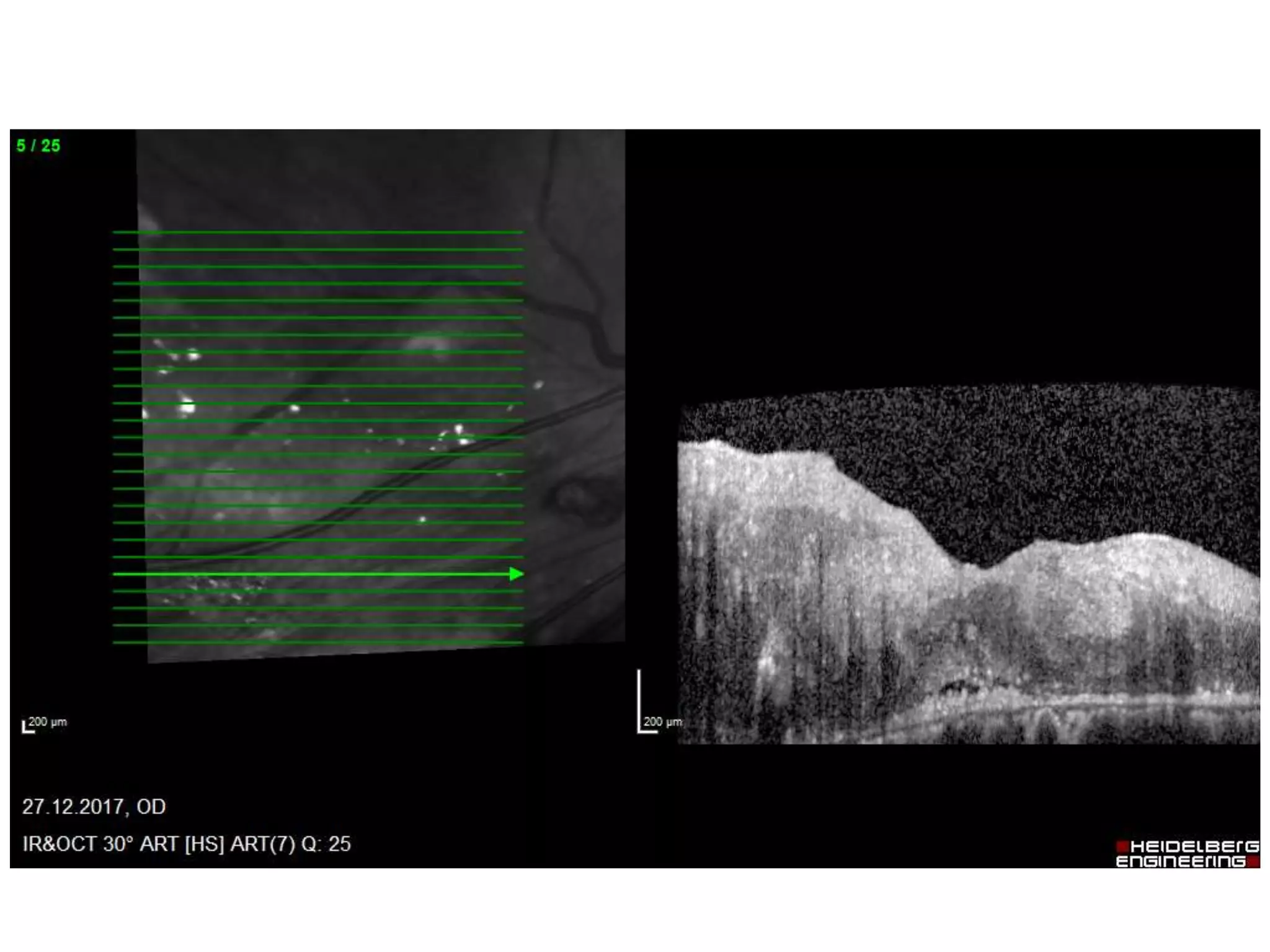
This document discusses familial exudative vitreoretinopathy (FEVR), a hereditary condition caused by defects in genes involved in retinal vascular development. It affects the peripheral retina and can cause retinal detachment. Clinical findings may include avascular areas, abnormal blood vessels, exudates, and retinal detachment. Diagnosis involves family history, examination findings, and imaging like fluorescein angiography. Treatment options depend on the stage and include laser, surgery like scleral buckling, and occasionally anti-VEGF injections. Long-term follow-up is needed as the condition is progressive and asymmetric between eyes. Family screening is also important to identify asymptomatic relatives.