1. The patient is a 75-year-old Thai man who fell off his bicycle 6 hours prior, injuring his left elbow and clavicle.
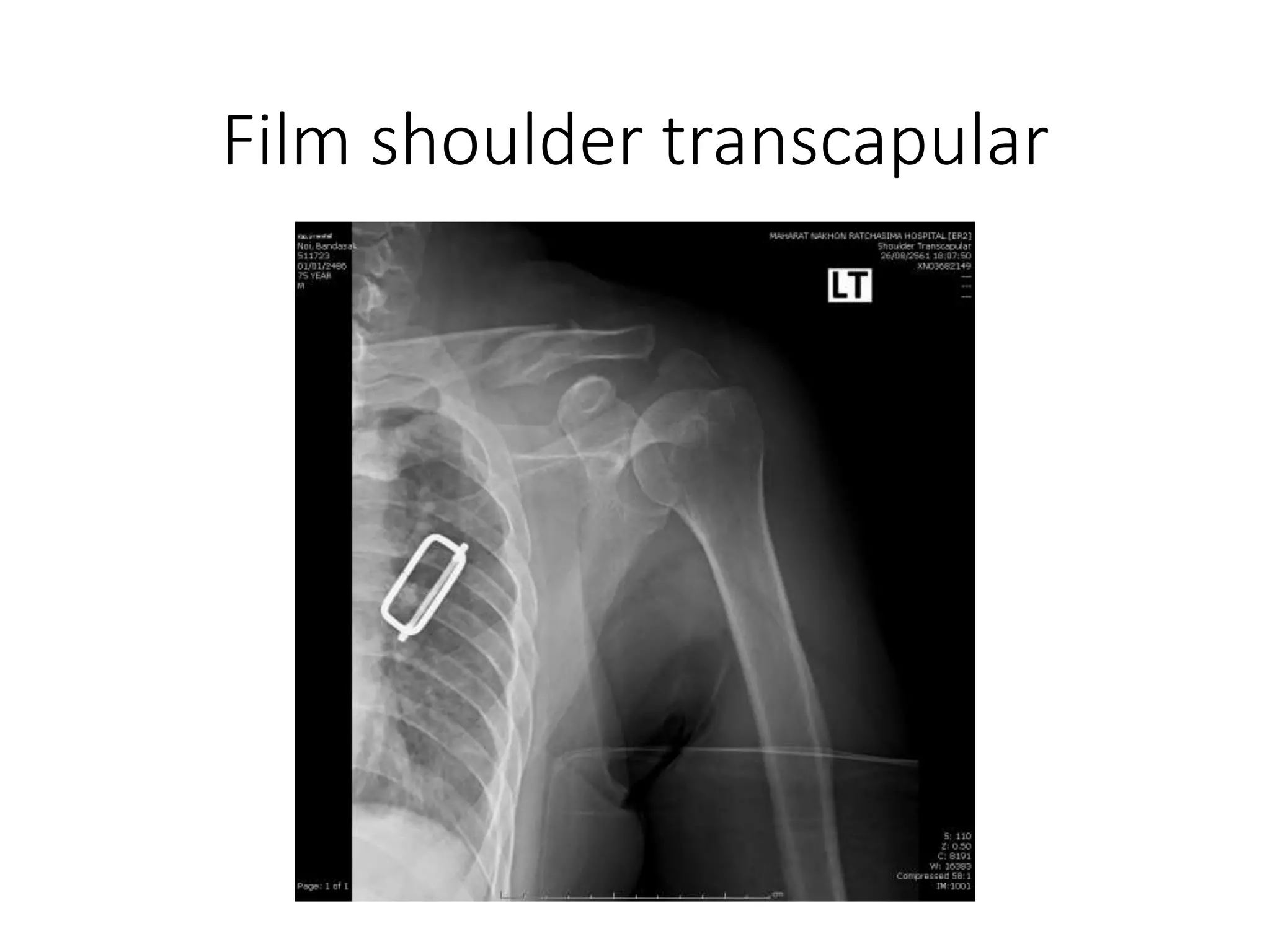
2. Radiographs show a fracture of the left shaft of the clavicle.
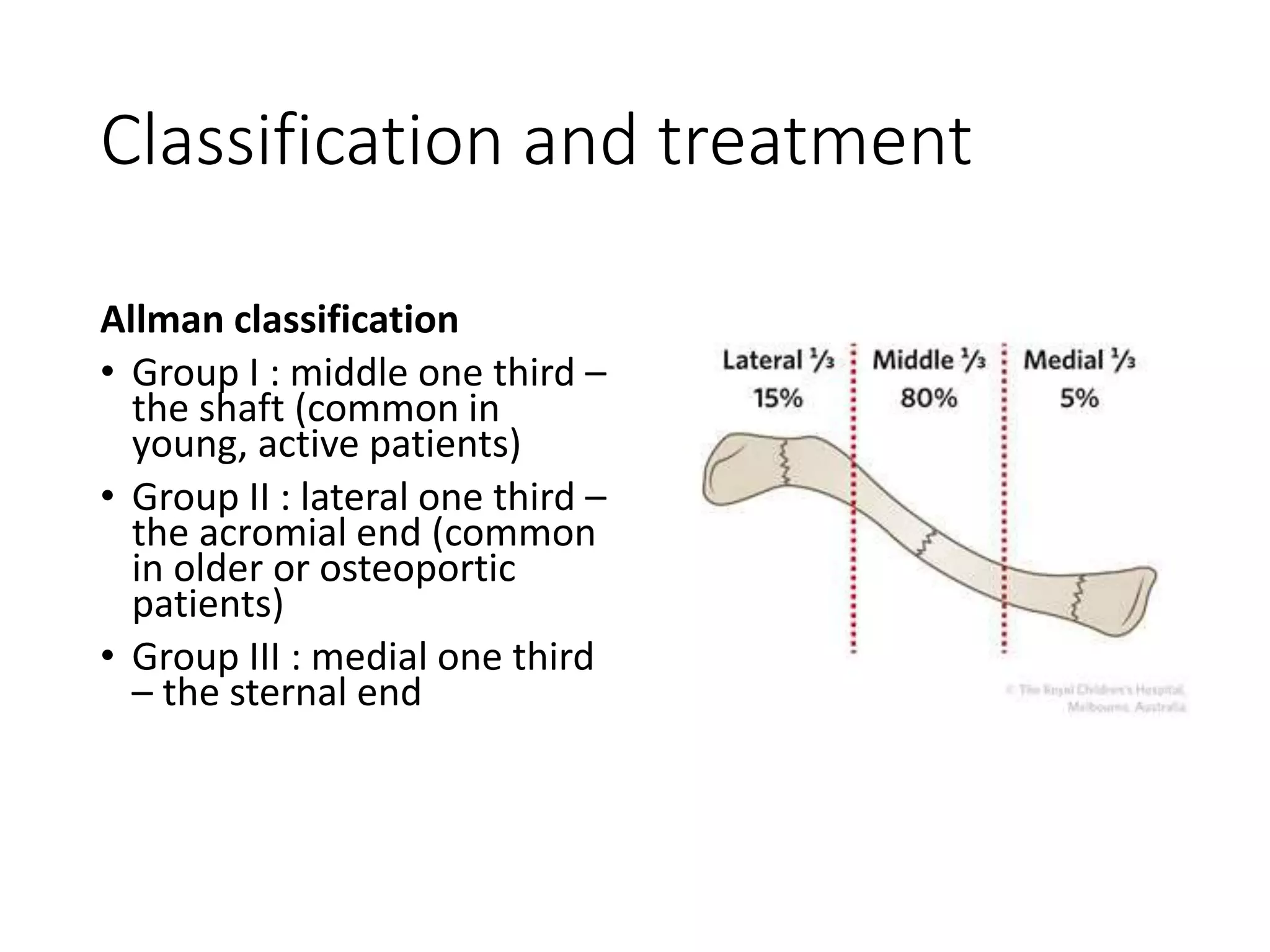
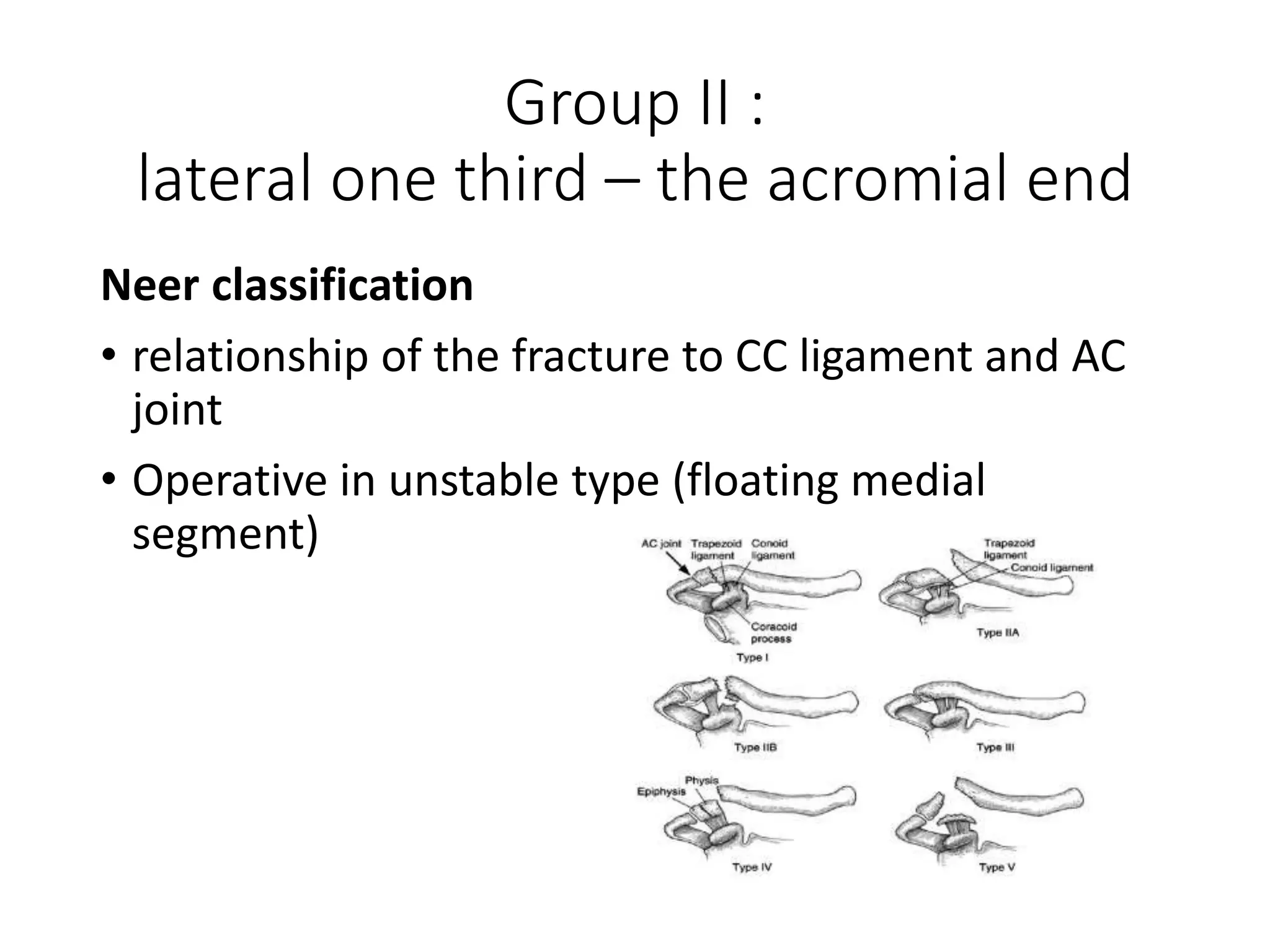
3. Clavicle fractures are commonly classified using the Allman or Neer classifications to determine appropriate treatment. Non-displaced or stable fractures are typically treated non-operatively while displaced or unstable fractures often require surgical fixation.