1) The patient is a 59-year-old Thai woman who fell and injured her left wrist. She was brought to the emergency department with a deformity and swelling of her left wrist.
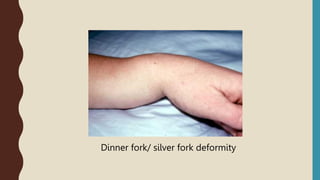
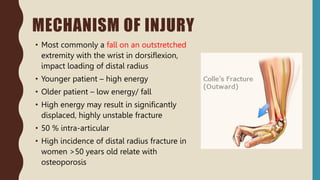
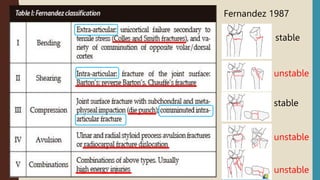
2) X-rays showed a fracture of the distal radius, known as a Colles' fracture.
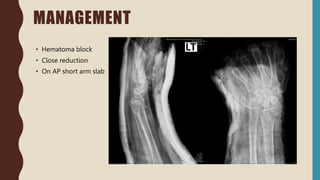
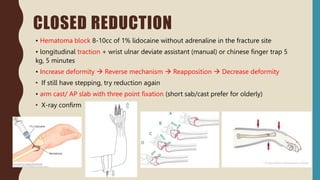
3) The fracture was treated with closed reduction, hematoma block, and application of a short arm splint.
The key points were that the patient fell and injured her left wrist, x-rays showed a Colles' fracture of the distal radius, and the fracture was treated non-operatively with closed reduction and splinting.