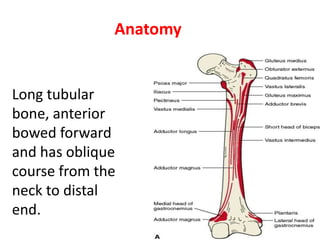
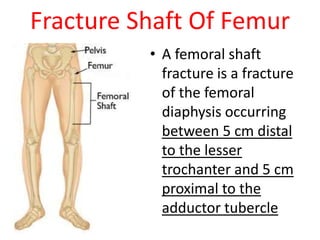
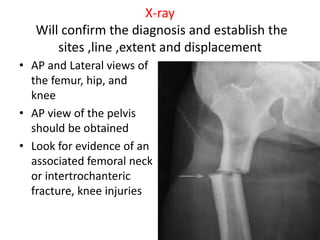
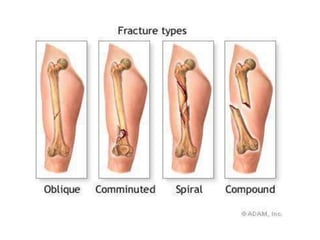
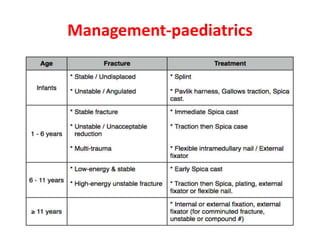
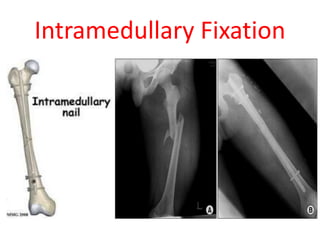
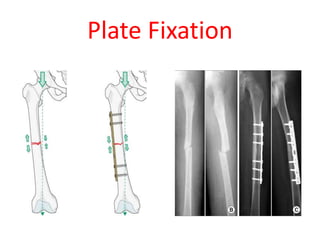
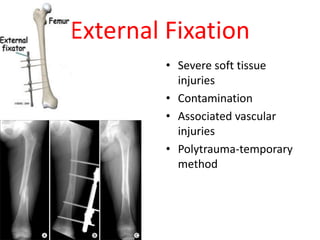
Femoral shaft fractures occur in the diaphysis of the femur between 5 cm distal to the lesser trochanter and 5 cm proximal to the adductor tubercle. They are commonly caused by high-energy trauma in young adults and falls in the elderly. Clinical evaluation involves assessing neurovascular status, associated injuries, and deformity or shortening of the leg. X-rays are used to confirm the diagnosis and classify the fracture. Treatment options include traction, casting, intramedullary nailing, plate fixation, or external fixation depending on the patient's age and the fracture pattern. Complications can include blood loss, nerve injuries, infections, and non-union.























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



