The document provides an overview of the digestive system, including its main functions and gross anatomy. It discusses the general tubular nature of the digestive tract and describes the individual organs that make up the system, such as the mouth, esophagus, stomach, and intestines. It also reviews the histological organization of the digestive tract walls into four main layers - mucosa, submucosa, muscularis externa, and serosa.
study of structures and functions of the gastrointestinal tract
- histology of the oral cavity
- histology of the pharynx
- histology of the esophagus and stomach
- histology of intestine
- histology of the liver and pancreas
study of structures and functions of the gastrointestinal tract
- histology of the oral cavity
- histology of the pharynx
- histology of the esophagus and stomach
- histology of intestine
- histology of the liver and pancreas
Histology of Gall bladder and its formation which consist of mainly 3 layers which they are:
- Mucosa
- Muscularis / Fibromuscular layer
- Serosa / Adventitia
And you must note that there is no Muscularis mucosa
& Submucosa inside Gall bladder...
Prepared by Nahry Omer Muhammad, University of Sulaimany/Collage of Medicine
The mucose membrane lining of gastrointestinal tract is stratified squamous epithelium at the esophagus which slowly convert into simple columnar epithelium at the stomach until the anus it converts back into the stratified squamous epithelium at the lower half of the anal canal. The stratified epithelium is a wear and tear epithelium.
As it passes down from the small to large intestine, goblet cells increase because as it passes down water was absorb, goblet cells function to produce mucous.
This is just a rough idea, for better slides with more reference please PM the author at davidgqf@gmail.com.
01.07.09(b): Tubular GI Tract - StomachOpen.Michigan
Slideshow is from the University of Michigan Medical School's M1 Gastrointestinal / Liver sequence
View additional course materials on Open.Michigan:
http://openmi.ch/med-m1gastro
Histology of Gall bladder and its formation which consist of mainly 3 layers which they are:
- Mucosa
- Muscularis / Fibromuscular layer
- Serosa / Adventitia
And you must note that there is no Muscularis mucosa
& Submucosa inside Gall bladder...
Prepared by Nahry Omer Muhammad, University of Sulaimany/Collage of Medicine
The mucose membrane lining of gastrointestinal tract is stratified squamous epithelium at the esophagus which slowly convert into simple columnar epithelium at the stomach until the anus it converts back into the stratified squamous epithelium at the lower half of the anal canal. The stratified epithelium is a wear and tear epithelium.
As it passes down from the small to large intestine, goblet cells increase because as it passes down water was absorb, goblet cells function to produce mucous.
This is just a rough idea, for better slides with more reference please PM the author at davidgqf@gmail.com.
01.07.09(b): Tubular GI Tract - StomachOpen.Michigan
Slideshow is from the University of Michigan Medical School's M1 Gastrointestinal / Liver sequence
View additional course materials on Open.Michigan:
http://openmi.ch/med-m1gastro
Histology/Micro Anatomy of Small Intestine.pptxMathew Joseph
The small intestine is an organ located in the gastrointestinal tract, between the stomach and the large intestine. It is, on average, 23ft long and is comprised of three structural parts; the duodenum, jejunum and ileum.
Functionally, the small intestine is chiefly involved in the digestion and absorption of nutrients. It receives pancreatic secretions and bile through the hepatopancreatic duct which aid with its functions.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Hemodialysis: Chapter 3, Dialysis Water Unit - Dr.Gawad
Chapter23 digestivepart1marieb
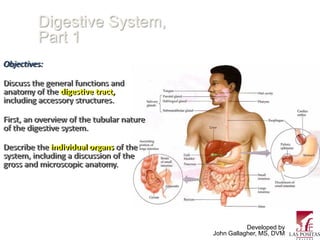
1. Digestive System,
Part 1
Objectives:
Discuss the general functions and
anatomy of the digestive tract,
including accessory structures.
First, an overview of the tubular nature
of the digestive system.
Describe the individual organs of the
system, including a discussion of the
gross and microscopic anatomy.
Developed by
John Gallagher, MS, DVM
2. Digestive System Overview
AKA:
Digestive Tract
Alimentary Tract or Canal
GI tract
Gut
Muscular, hollow tube,
from the lips to the anus
+
Various accessory organs
3. Digestive System Overview
The function of the system as a whole is
processing food in such a way that nutrients
can be absorbed and residues eliminated.
Individual parts
function in:
• Ingestion
• Propulsion
• Mechanical digestion and
segmentation
• Chemical and enzymatic digestion
• Secretion
• Absorption
• Compaction
• Excretion and elimination
(defecation)
4. Membranes
Peritoneum - generic serous membrane in
abdominal cavity
Parietal and Visceral Peritoneum
Retroperitoneal vs. (intra)peritoneal
Mesenteries - double sheets of peritoneum, surrounding and
suspending portions of the digestive organs
• Greater omentum - "fatty apron", hangs anteriorly from Fig. 22.6
stomach; double layer encloses fat
• Lesser omentum - between stomach and liver
• Mesentery proper - suspends and wraps the small intestine
• Mesocolon - suspends and wraps the colon, parts are
– transverse mesocolon
– sigmoid mesocolon
6. Structure of Small Intestinal Wall
Plicae circulares – circular pleats around the interior of the small
intestine
Villi – minute finger-like projections, contain capillaries & lacteals
Microvilli – sub-microscopic size, projections on single cells
Function of all three?
Crypts at bottom of
villi—Cell
regeneration
(mitosis)
Glands—mucus,
enzymes
7. Smooth Muscle, a
review
• One nucleus
• Nonstriated
– Actin and myosin present
• Slow, sustained
contraction
• Communication
– Varicosities
– Gap junctions
8. Histological
Organization
Tube made up of four
layers.
1. Mucosa
2. Submucosa
3. Muscularis externa
4. Serosa = Visceral
Peritoneum
Modifications along its
length as needed.
9. The 4 Layers of
the Gut
1) Mucosa
Epithelium - usually simple columnar epithelium with goblet cells;
may be stratified squamous if protection needed, e.g., esophagus
Lamina propria – areolar connective tissue deep to epithelium
Muscularis mucosae -produces folds - plicae (small intestine) or Fig 23.7
rugae (stomach)
10. The 4 Layers of
the Gut
2) Submucosa – made up of loose connective tissue
contains submucosal plexus and blood vessels
Fig 23.7
11. The 4 Layers of
the Gut
3) Muscularis externa – smooth muscle, usually two layers
(controlled by the myenteric plexus; source of peristalsis )
-
inner layer: circular
outer layer: longitudinal Fig 23.7
12. The 4 Layers of
the Gut
4) Serosa
visceral layer of mesentery (contiguous
with the peritoneum) or adventitia
depending on location
Fig 23.7
14. Oral
Cavity
• AKA buccal cavity or mouth - lined
with oral mucosa (type of epithelium
?)
• Lips = labia
– Labial frenulum
• Hard and soft palates - form roof of
mouth
• Tongue - skeletal muscle
– Lingual frenulum
• Salivary glands - three pairs
• Teeth
• Fauces = opening to pharynx
15. Types and Numbers of Teeth
Dental succession
Deciduous (1o, baby, milk)
teeth - 20, replaced by
Permanent teeth - 32 teeth
16. Structure of Teeth
Fig 23.14
Crown - exposed surface of tooth
Neck - boundary between root and crown
Enamel - outer surface
Dentin – bone-like, but noncellular
Pulp cavity - hollow with blood vessels and
nerves
Root canal - canal length of root
Gingival sulcus - where gum and tooth meet
Periodontal Ligament
17. Three pairs of Salivary Glands
1-1.5 L / day for
digestion (?)
lubrication (swallowing) moistening
(tasting)
• Parotid – lateral side of face,
anterior to ear, drain by parotid
duct to vestibule near 2nd
upper molar
• Submandibular – medial
surface of mandible – drain
near lingual frenulum drain
posterior to lower molars
• Sublingual – in floor of mouth -
drain near lingual frenulum
18. Mumps
Swollen, painful parotid salivary glands (parotitis) on one or both sides of
the face
Etiology: Mumps virus (Myxovirus)
Fever and sometimes orchitis, pancreatitis etc.
About 1/3 of infected people do not show symptoms
Effective vaccine (MMR) since 1967
19. Esophagus
• Lined with noncornified
stratified squamous epithelium
• Food boluses propelled by
peristalsis of both skeletal and
smooth muscle (gravity, too)
• Hiatus; lower esophageal
sphincter
• GERD
23. Histology of Stomach
Type of epithelium lining stomach?
Gastric pits – shallow pits, external half rapidly
reproduces for replacement
Gastric glands – deep in lamina propria, 3 types of
cells
1. Parietal cells (produce HCl and intrinsic
factor B12)
2. Chief cells (produce pepsinogen)
3. Enteroendocrine cells – G cells (several
hormones including gastrin which stimulates both
parietal and chief cells)
24. Ulcers
• Mucosal erosion of stomach or
duodenum
• GERD
• NSAIDs
• Helicobacter pylori
• Stress??
• Dx by
esophagogastroduodenoscopy
http://www.you
tube.com/watc
h?v=hm1nEP
HxJ0E