Downloaded 128 times

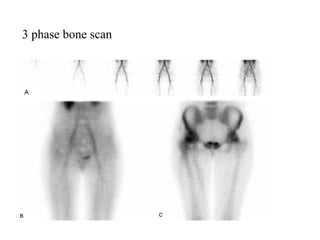
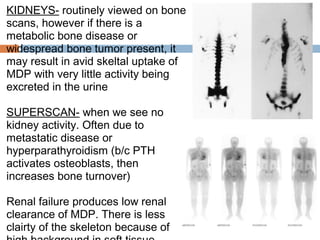
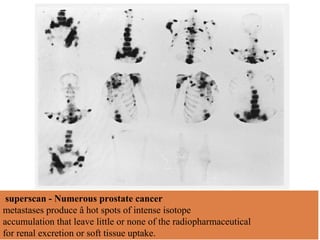


The bone scan is a nuclear medicine procedure that uses radiopharmaceuticals like technetium-99m to generate images of the skeletal system. It is useful for evaluating bone disorders and can detect abnormalities earlier than other imaging modalities. The scan involves injection of the radiotracer and acquisition of blood flow, blood pool, and bone scan phase images over hours. It is helpful for detecting fractures, metastases, infections and other bone abnormalities. Precise diagnosis may require correlation with clinical history and other imaging tests.





























































![[5]Isotope_Scan_Surgical_Diseases](https://cdn.slidesharecdn.com/ss_thumbnails/1664464-thumbnail.jpg?width=640&height=640&fit=bounds)






















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








