Downloaded 25 times


![100 Nuclear Medicine: The Requisites
bone scan is helpful in addressing several problems. The
most frequent indication for three-phase imaging is to
assess possible osteomyelitis. However, it is also beneficial
in the evaluation of the painful joint prosthesis, trauma,
bone graft status, and complex regional pain syndrome
(reflex sympathetic dystrophy). Dynamic scanning tech-nique
is summarized in Box 7-2.
If dynamic three-phase scanning is to be performed, a
bolus of Tc-99m MDP is injected intravenously with the
area in question under the camera. The injection site
should be chosen to avoid any suspected pathological con-dition.
For example, if comparison with the opposite hand
may be needed at any time, injection in a site such as the
foot should be considered. The first phase consists of serial
2- to 5-second dynamic images acquired for 60 seconds.
Then blood pool or soft tissue second-phase images are
Box 7-2. Three-Phase Skeletal Scintigraphy:
Protocol Summary
PREPARATION
Position gamma camera immediately over area
of concern.
RADIOPHARMACEUTICAL ADMINISTRATION
Administer intravenous bolus of Tc-99m methylene
diphosphonate using standard dosage.
FLOW PHASE
Obtain dynamic 2- to 5-second images for 60 seconds
after bolus injection.
BLOOD POOL AND TISSUE PHASE
Obtain immediate static images for time (5 minutes)
or counts (300k).
SKELETAL PHASE
Delayed 300k-1000k images at 2 to 4 hours.
obtained of the region and secondary areas of interest,
such as in patients with arthritis or multiple stress injuries.
Delayed images constitute the third phase of a three-phase
bone scan. Alternatively, delayed images are done
alone for routine studies, such as the assessment of meta-static
disease. The patient should be well hydrated, and
after injection the patient must be instructed to drink sev-eral
cups of fluid to improve background clearance. Fre-quent
voiding reduces radiation dose. Care must be used
because urinary contamination frequently causes confu-sion
or masks potential lesion sites. Although a delay of
2 hours may yield images of sufficient quality in younger
patients, waiting 3 or 4 hours after injection is often neces-sary
in the elderly and in those with poor renal function.
Images delayed further, at 24 hours, which is a fourth
phase, may be needed to clear soft tissue activity in the
most severe cases.
Using a low-energy, high-resolution collimator, delayed
planar images can be obtained by whole-body scan or
spot views. The whole-body scan allows rapid, seamless
coverage as the camera moves over the patient at a pre-determined
rate. Spot views, on the other hand, can pro-vide
greater detail because of higher resolution and can
better define pathological conditions by using different
camera positions. In most centers, a whole-body scan
is performed with high count spot views reserved for
symptomatic areas or additional views of suspicious-appearing
regions (Fig. 7-4).
Other modifications include magnified pinhole collima-tor
views, commonly used in cases of osteonecrosis of the
hips and trauma to the carpal bones. Pinhole images also
may be needed in children to better visualize the joints.
Three-dimensional assessment of the bones with SPECT
allows for high-contrast images that can be formatted in
transaxial, sagittal, and coronal planes. SPECT images
fused to CT or acquired on a SPECT/CT scanner are
sometimes much easier to interpret. Compared with planar
images, SPECT shows improved contrast of cold and hot
lesions, more precise localization, and better resolution
(Fig. 7-5). The ability to precisely localize a lesion on
Box 7-1. Whole-Body Survey and Single-Photon
Emission Computed Tomography Skeletal
Scintigraphy: Protocol Summary
PATIENT PREPARATION
Patient should be well hydrated.
Patient voids immediately before study and
frequently for next several hours.
Patient should remove metal objects (jewelry, coins,
keys) before imaging.
RADIOPHARMACEUTICAL ADMINISTRATION
Select injection site to avoid possible sites of
pathology.
Adult dose: 20 mCi (740 MBq), intravenously
Pediatric dose: Webster’s rule:
Adult dose × [(age + 1)/(age + 7)].
Minimum dose 1.08 mCi (40 MBq)
TIME OF IMAGING
Begin imaging 2-4 hours after tracer administration.
PROCEDURE
Capture anterior and posterior images of whole
skeleton.
Whole-body scan (table rate ≈ 10 cm/min)
Multiple spot views
300k-500k counts/image entire body or
time a 500k posterior chest view and image
remaining views for that amount of time
Detail spot areas of concern (1000k counts/image)
SINGLE-PHOTON EMISSION COMPUTED
TOMOGRAPHY
Attenuation correction with computed tomography
or external rods optional.
Acquisition: Contoured orbit, 128 × 128 matrix,
6-degree intervals, 15-30 sec/stop.
Reconstruction: Filtered back projection, Butter-worth
filter; cutoff 0.4, power 7 or iterative recon-struction.
*Selection of single-photon emission computed tomography
acquisition
and reconstruction parameters depends greatly on available
equipment and software.](https://image.slidesharecdn.com/7skeletal-141117030208-conversion-gate02/85/7-skeletal-3-320.jpg)





























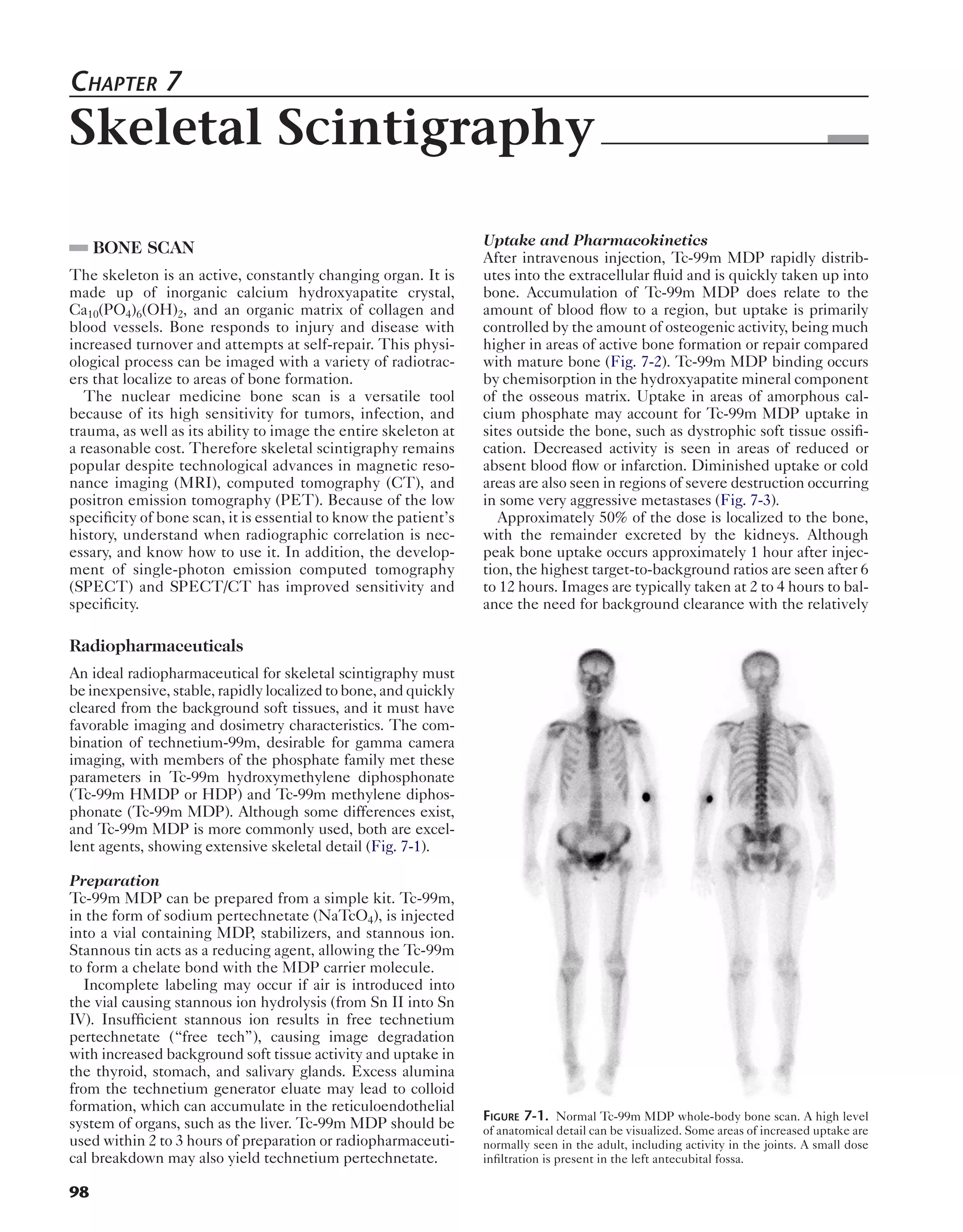
The document summarizes skeletal scintigraphy (bone scan) imaging. It describes how bone scan works by using radiotracers that localize to areas of bone formation/turnover. Technetium-99m methylene diphosphonate (Tc-99m MDP) is commonly used as it rapidly distributes to bone and is cleared from soft tissues. Imaging involves whole body scans 2-4 hours later to visualize bone abnormalities indicative of tumors, fractures or infections. Single photon emission computed tomography (SPECT) provides three-dimensional localization of lesions and improved specificity when fused to CT images. The distribution of uptake in normal bone changes with age and osteoarthritic changes are common benign findings.





































![[5]Isotope_Scan_Surgical_Diseases](https://cdn.slidesharecdn.com/ss_thumbnails/1664464-thumbnail.jpg?width=640&height=640&fit=bounds)

















































