Downloaded 146 times
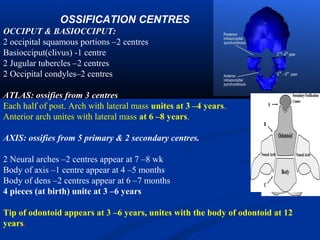

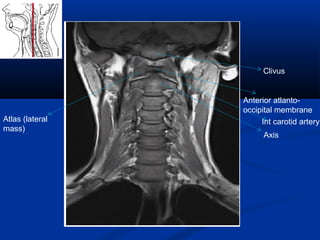
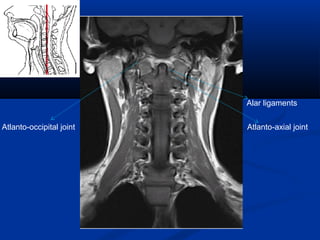
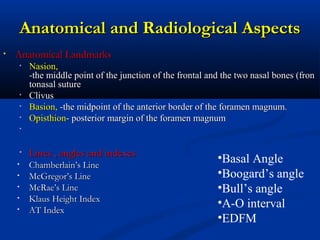
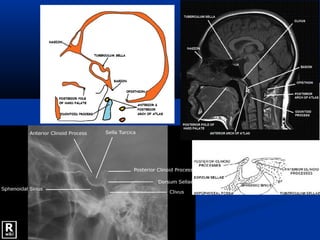

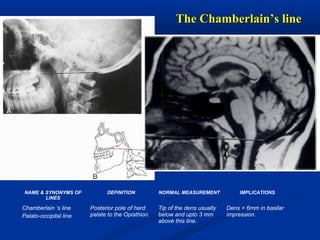


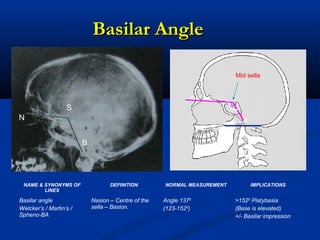
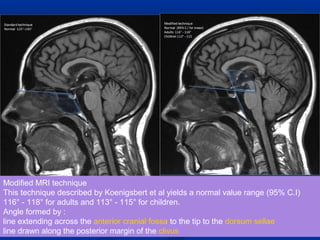
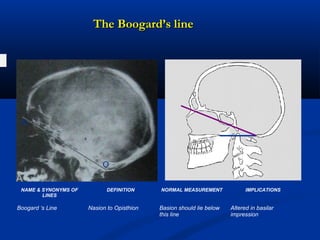
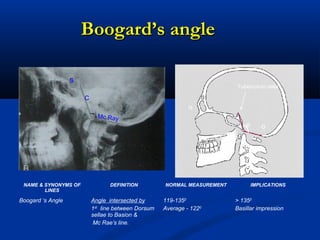
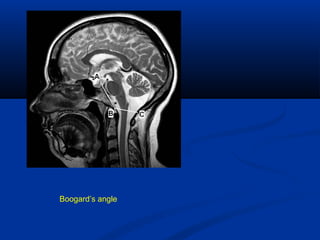
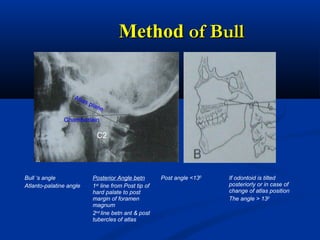
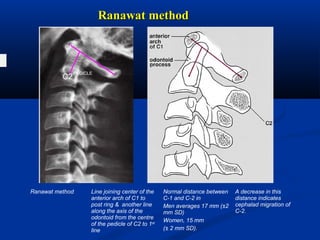
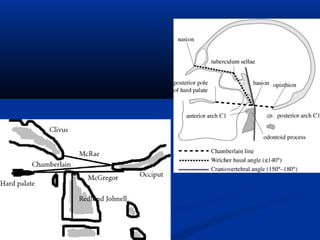
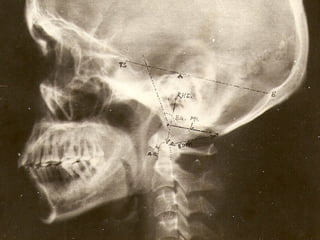
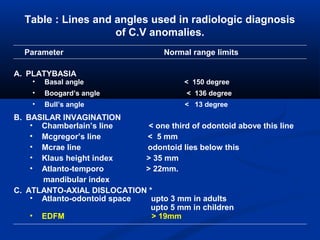
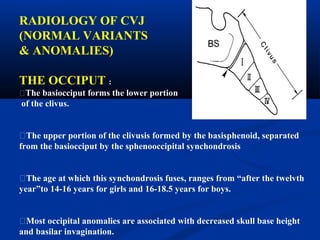
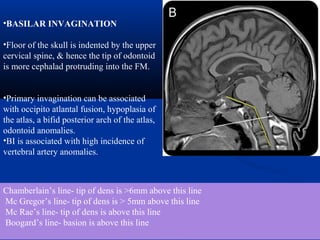



This document discusses cranio-vertebral anomalies and their classification. It begins by classifying bony and soft tissue anomalies. It then discusses the ossification centers of various bones including the occiput, atlas, and axis. Next, it covers the anatomical landmarks and radiological lines used to evaluate the cranio-vertebral junction, such as Chamberlain's line, McGregor's line, and the basilar angle. It provides the normal measurements for these lines. The document concludes by discussing radiological evaluation techniques including CT and MRI measurements.





























































































