Downloaded 301 times
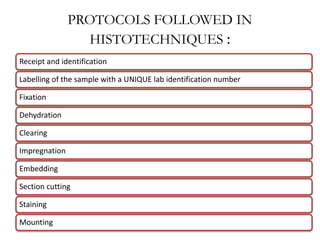






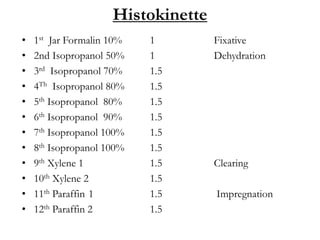



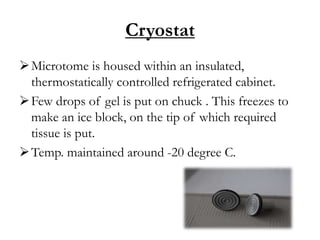


This document outlines the histotechnique process which tissues undergo before microscopic examination. Key steps include: fixation to preserve tissue structure; processing involving dehydration, clearing, and impregnation to allow sectioning; embedding tissues in paraffin blocks for microtomy; sectioning samples and staining, typically with hematoxylin and eosin, for visualization under the microscope. Finally, samples are mounted on slides and labeled for storage and pathological examination.











































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










