Downloaded 49 times
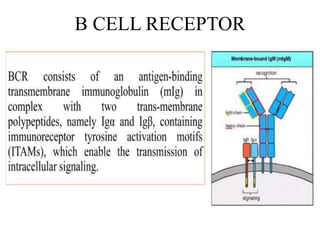
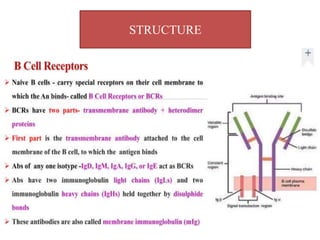
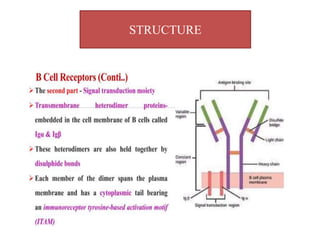
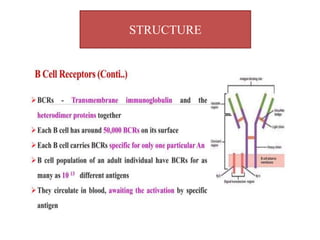
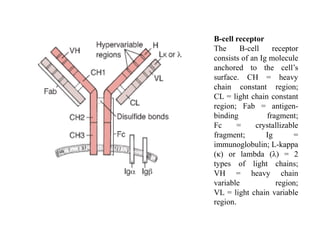
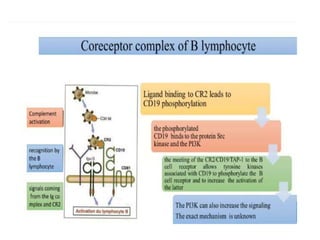
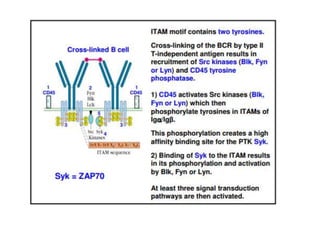
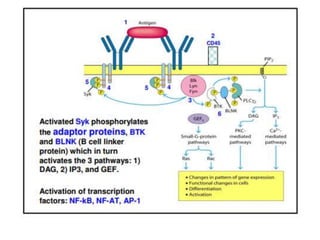
The B cell receptor is a transmembrane protein on B cells that is composed of a membrane-bound immunoglobulin molecule and a signal transduction moiety. The B cell receptor consists of an Ig molecule anchored to the cell's surface and has two key functions: signal transduction upon antigen interaction and internalization of antigens for processing and presentation to T cells. The B cell co-receptor is a complex of CD19, CD21, and CD81 expressed on mature B cells.























































































