AUXILIARY CRANE INSPECTION CHECKLIST Form # HSEQ - AC Rev 2.docx
•Download as DOCX, PDF•
0 likes•1,494 views

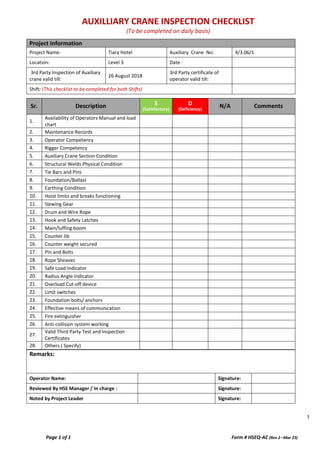
1. This document is an auxiliary crane inspection checklist for the Tiara Hotel Auxiliary Crane No. 4/3.06/1 located on Level 3. 2. It contains 28 items to check including the availability of manuals, maintenance records, operator and rigger competency, structural welds, foundation, hoist limits, drum and wire rope, hook, boom, counterweight, pins and bolts, sheaves, load indicators, limit switches, foundation bolts, means of communication, fire extinguisher, and anti-collision system. 3. The checklist notes that third party inspections of the crane and operator certificates are valid until August 26, 2018 and is to be completed for
Report
Share
Report
Share
Recommended
Overhead crane risk assessment
Lifting operation, as a huge and complicated systems engineering, involves every aspects of enterprise production. This paper will briefly introduce some common problems and control procedures during operation for occupational safety and health .
EOT Crane Inspection Check list, helpful for safety officers during inspection
it is for education and on the shop floor job for safety officers
LIFTING WORK PERMIT Form # HSEQ - LWP Rev 2.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Detail of Surroundings:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
Weight of Load : Max Height of Lift:
Max. Radius of Lift: Lifting Equipment ID/Registration No.:
Crane Capacity (SWL) Lift shall not be carried out if the load chart capacity exceeds 80% (Capacity …………)
Lifting Point Defined: ☐ Yes ☐ No
Road Closure/ Isolation required: ☐ Yes ☐ No
Underground services identified (if applicable):
☐ Yes ☐ No
Load Centre of Gravity Calculated: ☐ Yes ☐ No
3. Lifting Operation Details: (To be filled by initiator/originator)
Crane Operator Contact:
Rigger-1 Contact:
Rigger-2 Contact:
Type of Lifting Crane: ☐ Mobile Crane
☐ Wheel crane ☐ Crawler Crane
☐ All Terrain
☐ Loader/Hiab Crane
☐ Excavator
☐ Elevated working Platform
☐ Mobile Concrete Pump
☐ All Winch
☐ Other :
Lifting Crane Specification: ☐ Year of make (<25 years): __________
☐ Lifting Capacity: __________
☐ No. of rope fall wraps: ___________
☐ SWL: ______________
☐ Boom Reach: __________
☐ Fly Jib Reach: ___________
☐ Other(s): _____________
Type of lifting Gear(s): ☐ Chain Sling,
No. Of Legs: ___________
Each Leg Capacity: ____________
SWL: ______________
☐ Webbing Sling, SWL: ____________
☐ Wire Rope, SWL: _____________
☐ Lifting Beam, SWL: ___________
☐ Shackle, SWL: _____________
☐ Chain Blocks, SWL: ____________
☐ Hook with latch, SWL: ___________
☐ Eye Bolt/Nut, SWL: ____________
☐ Other(s): _________________
4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Risk assessment/ method statement and Lifting Plan developed, approved and communicated? ☐ ☐ ☐
Crane outriggers fully extended and spreading pads in place ☐ ☐ ☐
Operatives are consulted and trained? ☐ ☐ ☐
All wheels are off the ground. ☐ ☐ ☐
Provision of vigilance supervision? ☐ ☐ ☐
SWL and radius indicators in working order with visual and audible warning ☐ ☐ ☐
Has the crane valid certification ☐ ☐ ☐
Wind indicator is fitted & in working order ☐ ☐ ☐
Has the lifting gears valid certification ☐ ☐ ☐
load(s) slung correctly by a competent rigger ☐ ☐ ☐
Riggers/slinger competent and certified ☐ ☐ ☐
Tag-line(s) are connected with the load ☐ ☐ ☐
Correct crane selected for the load(s) and radius ☐ ☐ ☐
Suspended Load slewing path is cleared from people and barricaded ☐ ☐ ☐
Ground suitable, even, firm and prepared ☐ ☐ ☐
Destination of load(s) is cleared and prepared sufficiently ☐ ☐ ☐
Safe means of access/egress provided
Recommended
Overhead crane risk assessment
Lifting operation, as a huge and complicated systems engineering, involves every aspects of enterprise production. This paper will briefly introduce some common problems and control procedures during operation for occupational safety and health .
EOT Crane Inspection Check list, helpful for safety officers during inspection
it is for education and on the shop floor job for safety officers
LIFTING WORK PERMIT Form # HSEQ - LWP Rev 2.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Detail of Surroundings:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
Weight of Load : Max Height of Lift:
Max. Radius of Lift: Lifting Equipment ID/Registration No.:
Crane Capacity (SWL) Lift shall not be carried out if the load chart capacity exceeds 80% (Capacity …………)
Lifting Point Defined: ☐ Yes ☐ No
Road Closure/ Isolation required: ☐ Yes ☐ No
Underground services identified (if applicable):
☐ Yes ☐ No
Load Centre of Gravity Calculated: ☐ Yes ☐ No
3. Lifting Operation Details: (To be filled by initiator/originator)
Crane Operator Contact:
Rigger-1 Contact:
Rigger-2 Contact:
Type of Lifting Crane: ☐ Mobile Crane
☐ Wheel crane ☐ Crawler Crane
☐ All Terrain
☐ Loader/Hiab Crane
☐ Excavator
☐ Elevated working Platform
☐ Mobile Concrete Pump
☐ All Winch
☐ Other :
Lifting Crane Specification: ☐ Year of make (<25 years): __________
☐ Lifting Capacity: __________
☐ No. of rope fall wraps: ___________
☐ SWL: ______________
☐ Boom Reach: __________
☐ Fly Jib Reach: ___________
☐ Other(s): _____________
Type of lifting Gear(s): ☐ Chain Sling,
No. Of Legs: ___________
Each Leg Capacity: ____________
SWL: ______________
☐ Webbing Sling, SWL: ____________
☐ Wire Rope, SWL: _____________
☐ Lifting Beam, SWL: ___________
☐ Shackle, SWL: _____________
☐ Chain Blocks, SWL: ____________
☐ Hook with latch, SWL: ___________
☐ Eye Bolt/Nut, SWL: ____________
☐ Other(s): _________________
4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Risk assessment/ method statement and Lifting Plan developed, approved and communicated? ☐ ☐ ☐
Crane outriggers fully extended and spreading pads in place ☐ ☐ ☐
Operatives are consulted and trained? ☐ ☐ ☐
All wheels are off the ground. ☐ ☐ ☐
Provision of vigilance supervision? ☐ ☐ ☐
SWL and radius indicators in working order with visual and audible warning ☐ ☐ ☐
Has the crane valid certification ☐ ☐ ☐
Wind indicator is fitted & in working order ☐ ☐ ☐
Has the lifting gears valid certification ☐ ☐ ☐
load(s) slung correctly by a competent rigger ☐ ☐ ☐
Riggers/slinger competent and certified ☐ ☐ ☐
Tag-line(s) are connected with the load ☐ ☐ ☐
Correct crane selected for the load(s) and radius ☐ ☐ ☐
Suspended Load slewing path is cleared from people and barricaded ☐ ☐ ☐
Ground suitable, even, firm and prepared ☐ ☐ ☐
Destination of load(s) is cleared and prepared sufficiently ☐ ☐ ☐
Safe means of access/egress provided
Lifting Equipment Inspection
Schillings Hoisting Equipment is a leading supplier of quality lifting chains, lifting inspection, rigging & industrial products throughout Adelaide & SA.
TOWER CRANE INSPECTION CHECKLIST Form # HSEQ - TCI Rev 2 -.docx
Project Information
Project Name: Tower Crane No:
Location: Date :
3rd Party Inspection of Tower crane valid till: 3rd Party certificate of operator valid till:
Shift: (This checklist to be completed for both Shifts)
Sr. Description Yes No N/A Comments
1. Foundation bolts/ anchors
2. Main power disconnect switch
3. Hook sheaves/ swivel
4. Access ladders/ platforms
5. Section connecting bolts/ pins
6. Communication device (walkie talkie available/ working)
7. Hydraulic hoses for leaks
8. Gear boxes for oil level/ leaks
9. Slewing ring bolts
10. Counter weights secured
11. Wire rope condition
12. Control function
13. Hoist limits and breaks functioning
14. Booms lights working
15. Load chart
16. Fire extinguisher
17. Aircraft warning lights working
18. Sign boards secured
19. Radius mark signs secured
20. Anti-collision system working
21. Swivel Brakes removed before end of shift/ high wind
22. Riggers available
23. Condition of lifting tools ensured through riggers
24. Others ( Specify)
Remarks:
This checklist to be completed for both Shifts
Operator Name: Signature:
Reviewed By HSE Manager / In charge : Signature:
12 sheet piling operations (temporary works) risk assessment templates
12 Sheet Piling Operations (Temporary Works) Risk Assessment Templates
Sheet piling Rig checks on arrival to site
PRIOR TO USE
Access of rig and sheet pile delivery vehicles to work areas
Siting and setting up of sheet piling rig
Sheet piling operation
(Mobile rig Operator)
Sheet piling operation
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
Project Information
Project Name: Concrete Pump Reg. No:
Location: Operators Name:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Concrete Pump 3rd Party Certificate & Registration
2. Sonographic test of all pipes
3. Calibration of all the pressure gauges
4. Operator’s Competency Certificate & Driver’s License
5. Safe distance from the edge of the excavation
6. Outrigger pads are free from damage
7. Outriggers are level
8. Reverse alarm and beacon light are operational
9. Whip arrester on the pipes and pump
10. Safe access for concrete mixer to the area (In/Out)
11. Area properly barricaded and signage posted
12. Hydraulic Oil / Diesel Leakage
13. Extension Pipeline - Free from damage
14. Extension Pipeline -Locking pin in every connection
15. Extension Pipeline - Adequately supported & secured
16. Spillage control measure in place
17. Other accessories e.g. spider pacing boom 3rd party certificate
18. Static pumps positioned properly
19. Static pumps – concrete pipes fixed on structure as per design
20. Concrete pipes coupler pins provided
21. Concrete pipes on floor – away from scaffolds/ formworks
22. Competent banks man and supervision provided
23. Others (Specify)
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
Noted by Project Leader Signature:
Job Safety Analysis For Lifting Activity By Crane | JSA | Gaurav Singh Rajput
Job Safety Analysis For Lifting Activity By Crane | Gaurav Singh Rajput | TBRA | JSA | Risk Assessment
The Many Hazards Of Manual Cut and Bend Of Rebars
When it comes to rebar cutting, bending and welding
The risk of injuries is high especially since it is cut and bent manually by unskilled labour
This not only increases the chances of hazards but also results in inaccuracies and inefficiencies
9 lifting operations with tower crane risk assessment templates
9 Lifting Operations with Tower crane Risk Assessment Templates
Access of Tower crane sections to work areas
Tower crane foundations
Siting, setting up and testing of Tower crane
Lifting of equipment and material
(Tower crane Operator)
Tower Crane supervision
Jumping and dismantling of Tower Crane
3 emergency management risk assessment templates
3 Emergency Management Risk Assessment Templates
Emergency Procedure
Access requirement for Emergency Vehicles
• Police;
• Civil Defense;
• Ambulance;
(Including as per 2017 Fire Life Safety COP Requirements)
Reverse Parking of private vehicles office areas
Project Vehicle Parking
Project Emergency Site Exits
Project Emergency Communication
Project Assembly points
MAST CLIMBER & CRADLE PERMIT Form # HSEQ - Rev 2.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Area / Location of Mast Climber or Cradle:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
Serial No. of Mast Climber or Cradle: No. of persons working on Mast Climber or Cradle:
Safe Working Load of Mast Climber or Cradle:
Other(s):
3. Mast Climber or Cradle Operators Details: (To be filled by initiator/originator)
Operator Contact:
Rigger-1 Contact:
Rigger-2 Contact:
Rigger-3 Contact:
4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Risk assessment/ method statement developed, approved and communicated? ☐ ☐ ☐
Area below mast climber or cradle free from personnel and barriers in place when working? ☐ ☐ ☐
Mast climber or cradle have a valid 3rd party certificate and displayed? ☐ ☐ ☐
All mast climber or cradle rigging points secure to building? ☐ ☐ ☐
Operator competent and certified? ☐ ☐ ☐
Are the mast climber or cradles brakes working? ☐ ☐ ☐
Wire ropes in good conditions? ☐ ☐ ☐
Proper barricade and signage are posted? ☐ ☐ ☐
Counterweights sufficient and properly anchored/secured? ☐ ☐ ☐
Mast climber or cradle SWL displayed?
☐ ☐ ☐
Electrical wires are in good conditions and free from obstructions? ☐ ☐ ☐
Access and egress will be on ground level? ☐ ☐ ☐
Anchor point for safety harness available and in good condition? ☐ ☐ ☐
Rescue plan available and communicated? ☐ ☐ ☐
Personnel working in mast climber cradle wearing safety harness and clipped on? ☐ ☐ ☐
Others (specify): ☐ ☐ ☐
5. Acknowledgement by Initiator and Evaluator:
☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Date /Time
Comments (if any):
6. Authorization (PM/CM):
Name: Designation:
Signature: Date /Time:
7. Completion/Cancelation of Permit:
☐ Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
☐ Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
More Related Content
What's hot
Lifting Equipment Inspection
Schillings Hoisting Equipment is a leading supplier of quality lifting chains, lifting inspection, rigging & industrial products throughout Adelaide & SA.
TOWER CRANE INSPECTION CHECKLIST Form # HSEQ - TCI Rev 2 -.docx
Project Information
Project Name: Tower Crane No:
Location: Date :
3rd Party Inspection of Tower crane valid till: 3rd Party certificate of operator valid till:
Shift: (This checklist to be completed for both Shifts)
Sr. Description Yes No N/A Comments
1. Foundation bolts/ anchors
2. Main power disconnect switch
3. Hook sheaves/ swivel
4. Access ladders/ platforms
5. Section connecting bolts/ pins
6. Communication device (walkie talkie available/ working)
7. Hydraulic hoses for leaks
8. Gear boxes for oil level/ leaks
9. Slewing ring bolts
10. Counter weights secured
11. Wire rope condition
12. Control function
13. Hoist limits and breaks functioning
14. Booms lights working
15. Load chart
16. Fire extinguisher
17. Aircraft warning lights working
18. Sign boards secured
19. Radius mark signs secured
20. Anti-collision system working
21. Swivel Brakes removed before end of shift/ high wind
22. Riggers available
23. Condition of lifting tools ensured through riggers
24. Others ( Specify)
Remarks:
This checklist to be completed for both Shifts
Operator Name: Signature:
Reviewed By HSE Manager / In charge : Signature:
12 sheet piling operations (temporary works) risk assessment templates
12 Sheet Piling Operations (Temporary Works) Risk Assessment Templates
Sheet piling Rig checks on arrival to site
PRIOR TO USE
Access of rig and sheet pile delivery vehicles to work areas
Siting and setting up of sheet piling rig
Sheet piling operation
(Mobile rig Operator)
Sheet piling operation
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
Project Information
Project Name: Concrete Pump Reg. No:
Location: Operators Name:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Concrete Pump 3rd Party Certificate & Registration
2. Sonographic test of all pipes
3. Calibration of all the pressure gauges
4. Operator’s Competency Certificate & Driver’s License
5. Safe distance from the edge of the excavation
6. Outrigger pads are free from damage
7. Outriggers are level
8. Reverse alarm and beacon light are operational
9. Whip arrester on the pipes and pump
10. Safe access for concrete mixer to the area (In/Out)
11. Area properly barricaded and signage posted
12. Hydraulic Oil / Diesel Leakage
13. Extension Pipeline - Free from damage
14. Extension Pipeline -Locking pin in every connection
15. Extension Pipeline - Adequately supported & secured
16. Spillage control measure in place
17. Other accessories e.g. spider pacing boom 3rd party certificate
18. Static pumps positioned properly
19. Static pumps – concrete pipes fixed on structure as per design
20. Concrete pipes coupler pins provided
21. Concrete pipes on floor – away from scaffolds/ formworks
22. Competent banks man and supervision provided
23. Others (Specify)
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
Noted by Project Leader Signature:
Job Safety Analysis For Lifting Activity By Crane | JSA | Gaurav Singh Rajput
Job Safety Analysis For Lifting Activity By Crane | Gaurav Singh Rajput | TBRA | JSA | Risk Assessment
The Many Hazards Of Manual Cut and Bend Of Rebars
When it comes to rebar cutting, bending and welding
The risk of injuries is high especially since it is cut and bent manually by unskilled labour
This not only increases the chances of hazards but also results in inaccuracies and inefficiencies
9 lifting operations with tower crane risk assessment templates
9 Lifting Operations with Tower crane Risk Assessment Templates
Access of Tower crane sections to work areas
Tower crane foundations
Siting, setting up and testing of Tower crane
Lifting of equipment and material
(Tower crane Operator)
Tower Crane supervision
Jumping and dismantling of Tower Crane
3 emergency management risk assessment templates
3 Emergency Management Risk Assessment Templates
Emergency Procedure
Access requirement for Emergency Vehicles
• Police;
• Civil Defense;
• Ambulance;
(Including as per 2017 Fire Life Safety COP Requirements)
Reverse Parking of private vehicles office areas
Project Vehicle Parking
Project Emergency Site Exits
Project Emergency Communication
Project Assembly points
What's hot (20)
TOWER CRANE INSPECTION CHECKLIST Form # HSEQ - TCI Rev 2 -.docx
TOWER CRANE INSPECTION CHECKLIST Form # HSEQ - TCI Rev 2 -.docx
12 sheet piling operations (temporary works) risk assessment templates
12 sheet piling operations (temporary works) risk assessment templates
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
CONCRETE PUMP & EXTENSION PIPELINE Form # HSEQ - CPC Rev 2.docx
Job Safety Analysis For Lifting Activity By Crane | JSA | Gaurav Singh Rajput
Job Safety Analysis For Lifting Activity By Crane | JSA | Gaurav Singh Rajput
9 lifting operations with tower crane risk assessment templates
9 lifting operations with tower crane risk assessment templates
Similar to AUXILIARY CRANE INSPECTION CHECKLIST Form # HSEQ - AC Rev 2.docx
MAST CLIMBER & CRADLE PERMIT Form # HSEQ - Rev 2.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Area / Location of Mast Climber or Cradle:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
Serial No. of Mast Climber or Cradle: No. of persons working on Mast Climber or Cradle:
Safe Working Load of Mast Climber or Cradle:
Other(s):
3. Mast Climber or Cradle Operators Details: (To be filled by initiator/originator)
Operator Contact:
Rigger-1 Contact:
Rigger-2 Contact:
Rigger-3 Contact:
4. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Risk assessment/ method statement developed, approved and communicated? ☐ ☐ ☐
Area below mast climber or cradle free from personnel and barriers in place when working? ☐ ☐ ☐
Mast climber or cradle have a valid 3rd party certificate and displayed? ☐ ☐ ☐
All mast climber or cradle rigging points secure to building? ☐ ☐ ☐
Operator competent and certified? ☐ ☐ ☐
Are the mast climber or cradles brakes working? ☐ ☐ ☐
Wire ropes in good conditions? ☐ ☐ ☐
Proper barricade and signage are posted? ☐ ☐ ☐
Counterweights sufficient and properly anchored/secured? ☐ ☐ ☐
Mast climber or cradle SWL displayed?
☐ ☐ ☐
Electrical wires are in good conditions and free from obstructions? ☐ ☐ ☐
Access and egress will be on ground level? ☐ ☐ ☐
Anchor point for safety harness available and in good condition? ☐ ☐ ☐
Rescue plan available and communicated? ☐ ☐ ☐
Personnel working in mast climber cradle wearing safety harness and clipped on? ☐ ☐ ☐
Others (specify): ☐ ☐ ☐
5. Acknowledgement by Initiator and Evaluator:
☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Date /Time
Comments (if any):
6. Authorization (PM/CM):
Name: Designation:
Signature: Date /Time:
7. Completion/Cancelation of Permit:
☐ Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
☐ Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
2017 cranes_hoists_and_elevators_ codes_regulations.pdf
2017 cranes_hoists_and_elevators_ codes_regulations.pdf
How many things do you THiiiNK are possible with the magic of the Foot & Golf...
Keep and open mind nothing is new in this world ..
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Location / Area :
Panel No : Voltage:
Permit Validity:
Time (from): _______Hrs.
Time (To): __________Hrs.
Date:
3. Prerequisites: (To be filled by initiator/originator and verified by Evaluator)
No: Checks Yes-No-NA Checks Yes-No-NA
ENERGIZATION (“Power On”) ISOLATION (“Power Off”)
1. Safety tool box briefing done. ☐ ☐ ☐
Method statement/Risk assessment in place. ☐ ☐ ☐
2. Authorized personnel / operators available. ☐ ☐ ☐
Authorized personnel / operators available. ☐ ☐ ☐
3. Method statement/Risk assessment in place. ☐ ☐ ☐
Adjacent live areas protected. ☐ ☐ ☐
4. Safety Barriers in place and safety signage Displayed. ☐ ☐ ☐
PPE available, high voltage rubber gloves, Safety goggles and floor mat. ☐ ☐ ☐
5. Working area is well lighted. ☐ ☐ ☐
Isolation/Lock-out in place. ☐ ☐ ☐
6. Electrical instruments are available for any Purpose. ☐ ☐ ☐
Electrical circuits “proved” by calibrated Instrument and found out to be no power. ☐ ☐ ☐
7. Correct PPE available, high voltage rubber Gloves, safety goggles and floor mat. ☐ ☐ ☐
Unauthorized workers are cleared from the Area. ☐ ☐ ☐
8. Approved WIR for installation, testing and Termination are attached to the permit. ☐ ☐ ☐
Standby operatives in the event of contact With live circuits. ☐ ☐ ☐
9. Emergency light (Flashlight) available. ☐ ☐ ☐
Emergency light (Flashlight) available. ☐ ☐ ☐
10. Is live work absolutely necessary? ☐ ☐ ☐
Emergency response plan available ☐ ☐ ☐
11. Unauthorized workers are cleared from the area.
☐ ☐ ☐
Other ( Specify): ☒ ☐ ☐
12. Power cable route from panel board to plant & equipment has been checked ☐ ☐ ☐
13 Emergency response plan available ☐ ☐ ☐
14 Other ( Specify): ☐ ☐ ☐
4. Acknowledgement by Initiator and Evaluator:
☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Date /Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Date /Time:
6. Completion/Cancelation of Permit:
☐ Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
☐ Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
Failure analysis and redesign of shaft of overhead crane
This paper deals with the failure analysis and redesign of shaft of overhead crane having capacity 25 tonne.
There is problem of failure of the shaft in gear box which is mounted on the crane. The shaft breakage occurred
due to dynamic, alternating low tensile– compressive stresses and simultaneous torsional load.
An overhead crane is mechanical equipment for lifting and lowering a load and moving it horizontally, with the
hoisting mechanism which is an integral part of the machine.
To carry out the failure analysis of shaft it is necessary to model the shaft in any modelling software like PROE, CATIA etc. Then analysis of existing shaft is done analytically and with ANSYS11. The shaft is then
redesigned with suitable material available in data book of machine design and then analysis of new design of
shaft is done with the help of ANSYS-11 software.
Risk Assessment and Method Statement for Installation of Boardwalk in Dublin ...
Construction Safety DT117/4
AERODYNAMIC ANALYSIS OF RAMP TYPE VORTEX GENERATOR ON NACA 2215 AIRFOIL
https://www.irjet.net/archives/V10/i6/IRJET-V10I640.pdf
IRJET- Study on Different Estimation Methods of Propulsion Power for 60 Mts O...
https://www.irjet.net/archives/V5/i11/IRJET-V5I11174.pdf
Structural Health Monitoring of a Cable-Supported Zhejiang Bridge
Structural Health Monitoring (SHM) aims to give, at every moment during the life
of a structure, a diagnosis of the “state” of the constituent materials, of the different
parts, and of the full assembly of these parts constituting the structure as a whole. The
state of the structure must remain in the domain specified in the design, although this
can be altered by normal aging due to usage, by the action of the environment, and by
accidental events. Thanks to the time-dimension of monitoring, which makes it
possible to consider the full history database of the structure, and with the help of
Usage Monitoring, it can also provide a prognosis (evolution of damage, residual life,
etc.).
The Zhijiang Bridge is a cable-stayed bridge built recently over the Hangzhou Qiantang River. It
has an arched twin-tower space and a twin-cable plane structure. The integrated system of
structural health monitoring and intelligent management for Zhijiang Bridge includes an
information acquisition system, data management system, evaluation and decision-making system,
and application service system. The monitoring components include the working environment of and application service system. The monitoring components include the working environment of
the bridge and various factors that affect bridge safety. The integrated system also includes a
forecasting and decision-making module for real-time online evaluation, which provides warnings
and makes decisions based on the monitoring information. The monitoring information, evaluation
results, maintenance decisions, and warning information can be input simultaneously into the
bridge monitoring center and traffic emergency center to share the monitoring data. The
installation of long-term structural health monitoring (SHM) systems to long-span cable-supported
bridges has become a trend to monitor loading conditions, assess performance, detect damage, and
guide maintenance. SHM systems can be used to investigate highway loading, railway loading,
wind characteristics, and temperature effects.
Rj101 tower crane safety monitor user manual(e)
tower crane safety monitor offer zone protection, black-box, anti-collision
Similar to AUXILIARY CRANE INSPECTION CHECKLIST Form # HSEQ - AC Rev 2.docx (20)
MAST CLIMBER & CRADLE PERMIT Form # HSEQ - Rev 2.docx
MAST CLIMBER & CRADLE PERMIT Form # HSEQ - Rev 2.docx
2017 cranes_hoists_and_elevators_ codes_regulations.pdf
2017 cranes_hoists_and_elevators_ codes_regulations.pdf
How many things do you THiiiNK are possible with the magic of the Foot & Golf...
How many things do you THiiiNK are possible with the magic of the Foot & Golf...
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docx
LIVE ELECTRICAL WORK PERMIT Form # HSEQ - LEP Rev 2.docx
Failure analysis and redesign of shaft of overhead crane
Failure analysis and redesign of shaft of overhead crane
Risk Assessment and Method Statement for Installation of Boardwalk in Dublin ...
Risk Assessment and Method Statement for Installation of Boardwalk in Dublin ...
AERODYNAMIC ANALYSIS OF RAMP TYPE VORTEX GENERATOR ON NACA 2215 AIRFOIL
AERODYNAMIC ANALYSIS OF RAMP TYPE VORTEX GENERATOR ON NACA 2215 AIRFOIL
IRJET- Study on Different Estimation Methods of Propulsion Power for 60 Mts O...
IRJET- Study on Different Estimation Methods of Propulsion Power for 60 Mts O...
Structural Health Monitoring of a Cable-Supported Zhejiang Bridge
Structural Health Monitoring of a Cable-Supported Zhejiang Bridge
More from Dwarika Bhushan Sharma
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB.pdf
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB
3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP.pdf
3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP3-STOP FALLS, CLEAN UP, PICK UP, WIPE UP-STOP FALLS, CLEAN UP, PICK UP, WIPE UP
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK.pdf
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK 2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK
PRE-START BRIEFING Form # HSEQ - PSB Rev 2 -.docx
Project Information:
Project Name:
Location: Supervisor :
Company name : Date:
Task Description:
Before work starts, the following must be in place
Induction Supervision Test Certificates Communication in same language Method Statement Risk Assessment Permit To Work Area Lighting
SELECT HAZARDS SELECT CONTROLS
( Tick to identify the controls in place)
Fall from height Training Access Ladder Access Handrail Edge Protection Secure Ladder Adequate Work Platform Guards for Openings Safety Harness Life Lines
Others( Specify)
Manual Handling Training Check Weight Mechanical Aids Access Route Team Lifting Wrong method Right Method
Power tools Training Color code inspection tag Check Cable Wheel guards Safe plug & sockets Cable Protection Proper Scaffold Cable Overhead Rotatory part guards
Scaffold Scaffold Tag Edge Protection Check Overhead works Access Ladder Adequate Work Platform Weather condition Out riggers Ladder 3 feet above platform Safety Harness
SELECT HAZARDS SELECT CONTROLS
( Tick to identify the controls in place)
Risk Assessment
Lifting Plan Tag Lines Lifting points / hooks Banks man Load stability Check Lifting gear Examination /Inspection Sharp edges protected
Lifting operations Weather/ Wind Speed Ground conditions Exclusion zone Communication Loading/ unloading vehicles Spreader Beams Check Ground conditions Check outriggers Others
Fire Fire Extinguisher Fire Hose Fire Exit Assembly point others
Slip/Trip Clean before you go Barricade the waste Waste Management Clean Access Housekeeping Clean liquid spillage Access signs Maintain access/ Egress
PPE
Safety Harness
Safety Helmet Coveralls Hi vis Jacket Safety Shoe Face Shield Ear Protection
Dust mask Respiratory Equipment Life line/ harness anchorage Hand Gloves Goggles/ Glass
Pre start Briefing done by: Signature:
Reviewed By HSE Manager/ In charge: Signature:
FIRE PREVENTION REQUIREMENTS Form # HSEQ - Rev 2.docx
Code of Practice
C.O.P # 01
Fire Prevention Requirements
(Management of Combustible Materials & Electrical Inspections)
Rev. 01, Mar 23
SUB CONTRACTORS HSE CHECKLIST Form # HSEQ - SPSC Rev 2 -.docx
1. Project Information:
Project Name: Checklist No.:
Sub-Contractor/Company:
Date:
2. Task Details:
Description of Task:
Location / Area :
Number of Workers:
Task Duration:
Time (from): _______Hrs.
Time (To): __________Hrs.
Date:
3. Prerequisites:
Checks Yes-No-NA Checks Yes-No-NA
Safety induction done. ☐ ☐ ☐
Safety tool box talk done. ☐ ☐ ☐
Method statement/Risk assessment in place. ☐ ☐ ☐
Training on Risk Assessment/ Method Statement done ☐ ☐ ☐
Job Safety Analysis done. ☐ ☐ ☐
3 Month Safety Look Ahead in place ☐ ☐ ☐
Permit to Work obtained ☐ ☐ ☐
Site Supervisor available ☐ ☐ ☐
PPE Available ☐ ☐ ☐
Working area is well lighted ☐ ☐ ☐
Tools and equipment inspected and tagged ☐ ☐ ☐
Unsafe conditions rectified ☐ ☐ ☐
Pre-Start Checks completed ☐ ☐ ☐
Emergency procedures communicated ☐ ☐ ☐
Unauthorized workers are cleared from the area.
☐ ☐ ☐
Other ( Specify): ☐ ☐ ☐
4. Acknowledgement by Sub-Contractor:
☐ Acknowledge that all above precautions/ controls measures have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Date /Time:
Signature: Date /Time
STORE INSPECTION Form # HSEQ - Form 2 Rev 2.docx
Project Information
Project Name: Store No.
Location: Contact Person:
Company Name: Arabtec Construction LLC. Date:
Sr. Description Yes No N/A Comments
1. Is access to stores are restricted to authorized personnel only?
2. Are there clear spaces around racks and stacks of stored materials and are adequate gangways provided between them?
3. Are stacks and storage kept clear of light fittings and hot surfaces?
4. Are all stocks of flammable liquids kept in purpose-built flammable storage liquid stores?
5. Are storage areas generally cleaned and tidy?
6. Are flammable liquids kept away from all possible sources of ignition?
7. Emergency exit signs are available in right locations
8. Smoke detectors/fire alarm are visible and accessible.
9. Fire extinguishers are available are serviced regularly
10. Are free standing shelves and cupboards secured for stability?
11. Are heavy items stored at a suitable height?
12. Are chemical containers used for storage suitable and clearly labelled?
13. Is there adequate light in the storage area?
14. Are all small loose items secured in appropriate storage?
15. Are warning notices, prohibiting smoking and naked lights prominently displayed?
16. Others if any:
Remarks:
Inspected by: Signature:
Reviewed by Project Manager/HSE Manager Signature:
WITNESS STATEMENT FORM.docx
PROJECT:
LOCATION: DATE:
I (name)_____________________________________would like provide my statement as follows on.
I hereby acknowledge that the above statement are true to the best of my recollection, and that these are my very own written down by m myself s others _________Name and Signature________
Name : ____________________________ Signature: ______________________
Position: _________________________________________Date:_________________
PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docx
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
☐ Fatality ☐ Major Injury ☐ Minor Injury ☐ Property Damage ☐ Environmental ☐ Other
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
4. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
5. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Corporate Office Remarks:
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docx
1. Project Information: (To be filled by initiator/originator)
Project Name: Permit No.:
Project Location:
Requesting Contractor/Company
2. Permit Issuance Details: (To be filled by initiator/originator)
THIS PERMIT IS ONLY FOR ONE SHIFT AND NOT EXTENDABLE
Description of Task:
Detail of Surroundings:
Permit Validity:
Time (from): __________Hrs.
Time (To): __________Hrs.
Date:
3. Control Measures: (To be filled by initiator/originator and verified by Evaluator)
Checks Yes-No-NA Checks Yes-No-NA
Method statement & Risk assessment developed, approved & communicated? ☐ ☐ ☐
Availability of rescue procedure and equipment? ☐ ☐ ☐
Operatives are trained and competent? ☐ ☐ ☐
Workplace appropriately illuminated ☐ ☐ ☐
Any high risk activity associated that requires PTW (i.e. hot work, CSE)? ☐ ☐ ☐
Forced ventilation provided? ☐ ☐ ☐
Are all necessary Permit approved and displayed at work location? ☐ ☐ ☐
Means of communication available? (Mobile, radio etc.) ☐ ☐ ☐
Safe access / Working Platform provided? ☐ ☐ ☐
Mandatory/specific good condition PPEs are available ☐ ☐ ☐
Availability of barricades/protection to prevent unauthorized or accidental entry? ☐ ☐ ☐
Life Line provided? ☐ ☐ ☐
Warning signs posted? ☐ ☐ ☐
Fall Protection equipment (e.g. full body harness) available? ☐ ☐ ☐
Availability of Fall protection arrangement? ☐ ☐ ☐
Other(s): ☐ ☐ ☐
Adequate Lighting provided? ☐ ☐ ☐
☐ ☐ ☐
4. Acknowledgement by Initiator and Evaluator:
☐ Acknowledge that all above precautions have been taken. These have also been fully explained to the operatives, and I consider them competent to do it safely.
Initiator/Originator Name: Designation:
Signature: Time:
☐ Acknowledge that I have checked above control measures and consider the work area safe to carry out the activity
Evaluator (HSE Team): Designation:
Signature: Time
Comments (if any):
5. Authorization (PM/CM):
Name: Designation:
Signature: Time:
6. Completion/Cancelation of Permit:
☐ Acknowledge that the area have been restored to a safe and orderly condition.
Initiator Signature: Time:
☐ Acknowledge that I have checked the area and been restored to a safe and orderly condition.
Evaluator Signature: Time:
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docx
Project Information
Project Name:
Date: Location:
Sr. Equipment type / Name Registration No & Exp Date Company Name
Operator Name / Mb. No Operator Third party competency certificate expiry date Operator License expiry date Equipment & Plant 3rd Party Inspection Certificate expiry date SWL / Capacity Signalman /Rigger name & TPC Exp Comment
1
2
3
4
5
6
7
8
9
10.
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge: Signature:
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docx
Accommodation Name: Date :
Accommodation Location: Time :
SN Description Yes NO N/A Observation Control
Measures Due Date
ACCESS AND EGRESS
1 Is there segregation between vehicles/ pedestrians
2 Is entry to inside camp restricted to workforce only? How is this controlled
3 Is the entrance well lit
4 Is the entrance free from water pooling
GENERAL HOUSEKEEPING
1 Are there adequate dustbins available? Are they covered
2 Is garbage disposed of on a regular basis?
3 Are toilets wash areas cleaned regular?
4 Is there adequate water for toilet and bath
5 Are water tanks kept covered at all times
6 Is soap and hand towels available?
7 Is bathroom area cleaned on a regular basis and kept dry and non-slippery
8 Is the water tank cleaned on a regular basis
9 Is the laundry area electrical & connections/ wires are in good condition.
10 Is the laundry area kept clean and dry
11 Is the tumble dryer filters cleaned frequently to prevent overheating
SEPTIC TANKS
1 Is the camp on main drainage?
2 If not are septic tanks provided?
3 Are septic tanks fitted with overflow alarm if not how are they prevented from overflowing
4 If septic tank in ground is it in a membrane?
5 If above ground is it protected from being hit by vehicular traffic?
FOOD PREPARATION AREA
1 Is the area kept clean and tidy
2 Are food preparation areas cleaned and free from cracks
3 Are signs for "No smoking" being posted
4 Food waste storage area is cleaned, odour free. Flies area controlled
5 Floor drains are provided in sink area
6 All refrigerators and freezers are working at correct temperatures Refrigerators 1c0 to 4c0
Freezers -14c0 to -18c0
7 Are there temp gauges fitted?
8 Are these temperatures recorded?
9 The Dining and Kitchen areas have an overall clean, tidy and well maintained appearance
10 LPG cylinders are of good conditions (free of damages)
11 Is storage of LPG satisfactory under shed & outside kitchens with no flammable materials nearby
12 Are Piping not perished
13 Are firefighting equipment provided in kitchen area?
LIVING QUARTERS
1 Are Ventilation working well
2 Is lighting suitable
3 Are Emergency numbers being posted in each room
4 Are emergency procedures posted in each room
5 Are Electrical sockets in good condition not damaged & no bare wires are placed in sockets
6 Are sockets overloaded
7 ELCB is provided checks carried out and recorded by
INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docx
INCIDENT INVESTIGATION REPORT
(To be submitted to the HSEQ Corporate Office within 7 days of incident.)
1. Project Information:
Project Name: Click here to enter text.
Report No.: Click here to enter text.
Project Location: Click here to enter text.
Property No.: Click here to enter text.
☐ Fatality ☐ Major Incident ☐ Minor Incident
2. Describe the Incident in detail:
Answer who, what, why, where, when & how in this section: (Attach additional pages if required)
Click here to enter text.
☐ Photos Attached
3. Incident Root Causes:
Describe direct, indirect & root cause: (Attach additional pages if required)
Click here to enter text.
4. Key Corrective Actions to Prevent Recurrence:
Describe the corrective actions with timeframe: (Attach additional pages if required)
Click here to enter text.
5. Key Corrections Taken Immediately after the Incident:
Attach additional pages if more space is required:
Click here to enter text.
6. Witnesses:
I declare that I witnessed the incident and the information provided above is true, correct and complete.
No. Name Designation Signature Date
1. Click here to enter text.
Click here to enter text.
Click here to enter text.
2. Click here to enter text.
Click here to enter text.
Click here to enter text.
7. Incident Information:
Initial Incident Report No.: Click here to enter text.
Date Reported: Click here to enter text.
Date of Incident: Click here to enter text.
Time of Incident: Click here to enter text.
Type of Incident: ☐ Near Miss
☐ Major Environmental Incident
☐ Serious Dangerous Occurrence
☐ Equipment / Property Damage
☐ Medical Treatment Case (MTC)
☐ Restricted Work Case (RWC)
☐ Lost Workday Case (LWC)
☐ Serious Occupational Illness/Disease
☐ Class 1 Injuries
☐ Permanent Partial Disability (PPD)
☐ Permanent Total Disability (PTD)
☐ Fatality (F)
Recordkeeping: ☐ Reportable ☐ Recordable
Incident Location on Site: Click here to enter text.
Applicable Reports: ☐ Police
☐ Medical
☐ Other (Specify)
Click here to enter text.
Attached: ☐ Yes ☐ No
☐ Yes ☐ No
☐ Yes ☐ No
8. Injured Person’s Personal Details:
In case of an incident with more than one injured person, complete the information for each person using separate forms.
Name: Click here to enter text.
Occupation: Click here to enter text.
Company: Click here to enter text.
MB / Oracle No.: Click here to enter text.
Nationality: Click here to enter text.
Date of Birth: Click here to enter text.
Passport Number: Click here to enter text.
Length of Service: Click here to enter text.
Gender: ☐ Male ☐ Female
Labour Card No.: Click here to enter text.
9. Incident Causes Details: To be supported with factual evidence
Immediate Cause
(Unsafe Acts) ☐ Failure to secure
☐ Failure to warn
☐ Removing / Defeating Safety Devices
☐
HSE INDUCTION Form # HSEQ - HSEI Rev 2 -.doc
HSE INDUCTION
(Workers)
Name: _________________________________ Trade: ____________________________
M.B. No./Company Name : ________________
Date of Joining: __________________________
SL. N SUBJECT ON INDUCTION PREVIOUS SAFETY EXPOSURE FURTHER SAFETY TRAINING NEED ANALYSIS
1. Introduction Safety Requirements
2. Working Safety is of Primary Importance
3. General Safety Rules
4. Basic Safety Requirements
5. House Keeping
6. Health, Hygiene & Welfare Facilities
7. Fire Extinguisher / Fire Fighting
8. Emergency Procedure
9. Safety Violations & Penalty
10. Safety Award
11. Manual Handling
Induction Given By: Name: ___________________________
Designation: ___________________________
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.doc
1st Warning 0 Ref. No. ______________
2nd Warning 0
3rd Warning 0
4th Warning 0 Date: ________________
Employee’s Name : ______________________________________ M.B No. : __________
Occupation : _____________________________________________________________________
Location / Project Site: _____________________________________________________________________
You have committed the following HSE violation/s:
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….….
The employee is hereby warned that if the violation is repeated further disciplinary action can be
taken as per the company Code of Conduct.
ORIGINATOR APPROVED BY (MANAGER IN CHARGE / ARABTEC HSEQ & ORG. RISK Manager)
Name: _______________________________ Name: _____________________________
Designation: _______________________________ Designation: _____________________________
Signature:
_______________________________ Signature:
_____________________________
Employee Acknowledgement:
I the undersigned have received this Safety warning letter / disciplinary notice and I admit that I have understood the contents.
0 Received on: ………………………….. (Date) Signature: ………………………………..…..
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docx
Project Information
Project Name: Porta Cabin No:
Location: Contact Person:
Company Name: Date :
Sr. Description Yes No N/A Comments
1. Emergency exit signs are available in right locations
2. Fire alarms and fire extinguishers are visible and accessible.
3. Fire doors (e.g. in stairways) are kept closed unless equipped with automatic closing device
4. Fire extinguishers are serviced regularly
5. Corridors and stairways are kept free of obstruction
6. Fire escape/ evacuation plan available and posted
7. First aid box available
8. Floor surfaces are kept dry and free of slip hazards
9. Electrical cords and plugs are in good condition with proper Grounding
10. Kitchen equipment checked
11. Fire blanket available in the pantry
12. Heat detector available in the pantry
13. Toilets floor clean and dry
14. Are staff trained to use Fire Extinguishers
15. Hand wash/ soap solution available in the toilet
16. Civil Defense or Authority approval
17. Others if any:
Remarks:
Inspected By: Signature:
Reviewed By HSE Manager / In charge : Signature:
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docx
MEDICAL REPORT FORM
Day _____________
Date ____________
Time ____________
To: _________________________________________________________________________________________________________
Dear Sir,
We would kindly request you to give necessary treatment to our following employee who had met with an accident and provide us with your diagnosis.
Name of injured __________________________________________________________ Age ( ) years.
Occupation __________________________________________________________ M.B. No. _______________________________
Date of Accident ____________________________________________ Time of Accident __________________________________
Place of Accident (Project Name) _______________________________ Location _________________________________________
Nature of Accident ____________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
First Aider Name: ________________________________ SE Manager/Incharge: ________________________________
Signature: ________________________________ Signature: ________________________________
(If Medical Certificate is attached, this portion is not required.)
MEDICAL REPORT
Nature and extent of Accident / Injury____________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Fit for duty___________________________________________________________________________________________________
Unfit for duty_________________________________________________________________________________________________
Remarks_____________________________________________________________________________________________________
____________________________________________________________________________________________________________
Signature of Medical Officer Date _______________
More from Dwarika Bhushan Sharma (20)
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB.pdf
5 - CLOWNS BELONG IN THE CIRCUS & NOT ON THE JOB.pdf
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK.pdf
2-THERE'S A SAFE WAY TO DO EVERY JOB, OF YOU DON'T KNOW ASK.pdf
FIRE PREVENTION REQUIREMENTS Form # HSEQ - Rev 2.docx
FIRE PREVENTION REQUIREMENTS Form # HSEQ - Rev 2.docx
SUB CONTRACTORS HSE CHECKLIST Form # HSEQ - SPSC Rev 2 -.docx
SUB CONTRACTORS HSE CHECKLIST Form # HSEQ - SPSC Rev 2 -.docx
PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docx
PROJECT LEADER INCIDENT BRIEFING Form # HSEQ - PLIB Rev 2 -.docx
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docx
LIFT SHAFT ENTRY PERMIT Form # HSEQ - LSEP Rev 2 -.docx
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docx
MOBILE PLANT REGISTER Form # HSEQ - MPR Rev 3.docx
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docx
LABOR ACCOMMODATION CHECKLIST Form # HSEQ - LAC Rev 2.docx
INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docx
INCIDENT INVESTIGATION REPORT Form # HSEQ - IIR Rev 9 -.docx
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.doc
HSE WARNING LETTER-DISCIPLINARY NOTICE Form # HSEQ - HSEWL Rev 6.doc
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docx
OFFICE PORTA CABIN INSPECTION Form # HSEQ - OPC Rev 2.docx
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docx
MEDICAL REPORT FORM Form # HSEQ - MRF Rev 3 -.docx
Recently uploaded
Quality defects in TMT Bars, Possible causes and Potential Solutions.
Maintaining high-quality standards in the production of TMT bars is crucial for ensuring structural integrity in construction. Addressing common defects through careful monitoring, standardized processes, and advanced technology can significantly improve the quality of TMT bars. Continuous training and adherence to quality control measures will also play a pivotal role in minimizing these defects.
Standard Reomte Control Interface - Neometrix
About
Indigenized remote control interface card suitable for MAFI system CCR equipment. Compatible for IDM8000 CCR. Backplane mounted serial and TCP/Ethernet communication module for CCR remote access. IDM 8000 CCR remote control on serial and TCP protocol.
• Remote control: Parallel or serial interface.
• Compatible with MAFI CCR system.
• Compatible with IDM8000 CCR.
• Compatible with Backplane mount serial communication.
• Compatible with commercial and Defence aviation CCR system.
• Remote control system for accessing CCR and allied system over serial or TCP.
• Indigenized local Support/presence in India.
• Easy in configuration using DIP switches.
Technical Specifications
Indigenized remote control interface card suitable for MAFI system CCR equipment. Compatible for IDM8000 CCR. Backplane mounted serial and TCP/Ethernet communication module for CCR remote access. IDM 8000 CCR remote control on serial and TCP protocol.
Key Features
Indigenized remote control interface card suitable for MAFI system CCR equipment. Compatible for IDM8000 CCR. Backplane mounted serial and TCP/Ethernet communication module for CCR remote access. IDM 8000 CCR remote control on serial and TCP protocol.
• Remote control: Parallel or serial interface
• Compatible with MAFI CCR system
• Copatiable with IDM8000 CCR
• Compatible with Backplane mount serial communication.
• Compatible with commercial and Defence aviation CCR system.
• Remote control system for accessing CCR and allied system over serial or TCP.
• Indigenized local Support/presence in India.
Application
• Remote control: Parallel or serial interface.
• Compatible with MAFI CCR system.
• Compatible with IDM8000 CCR.
• Compatible with Backplane mount serial communication.
• Compatible with commercial and Defence aviation CCR system.
• Remote control system for accessing CCR and allied system over serial or TCP.
• Indigenized local Support/presence in India.
• Easy in configuration using DIP switches.
HYDROPOWER - Hydroelectric power generation
Overview of the fundamental roles in Hydropower generation and the components involved in wider Electrical Engineering.
This paper presents the design and construction of hydroelectric dams from the hydrologist’s survey of the valley before construction, all aspects and involved disciplines, fluid dynamics, structural engineering, generation and mains frequency regulation to the very transmission of power through the network in the United Kingdom.
Author: Robbie Edward Sayers
Collaborators and co editors: Charlie Sims and Connor Healey.
(C) 2024 Robbie E. Sayers
Halogenation process of chemical process industries
This presentation is about nitration process of industries, unit processes of chemical engineering.
NO1 Uk best vashikaran specialist in delhi vashikaran baba near me online vas...
NO1 Uk best vashikaran specialist in delhi vashikaran baba near me online vas...Amil Baba Dawood bangali
Contact with Dawood Bhai Just call on +92322-6382012 and we'll help you. We'll solve all your problems within 12 to 24 hours and with 101% guarantee and with astrology systematic. If you want to take any personal or professional advice then also you can call us on +92322-6382012 , ONLINE LOVE PROBLEM & Other all types of Daily Life Problem's.Then CALL or WHATSAPP us on +92322-6382012 and Get all these problems solutions here by Amil Baba DAWOOD BANGALI
#vashikaranspecialist #astrologer #palmistry #amliyaat #taweez #manpasandshadi #horoscope #spiritual #lovelife #lovespell #marriagespell#aamilbabainpakistan #amilbabainkarachi #powerfullblackmagicspell #kalajadumantarspecialist #realamilbaba #AmilbabainPakistan #astrologerincanada #astrologerindubai #lovespellsmaster #kalajaduspecialist #lovespellsthatwork #aamilbabainlahore#blackmagicformarriage #aamilbaba #kalajadu #kalailam #taweez #wazifaexpert #jadumantar #vashikaranspecialist #astrologer #palmistry #amliyaat #taweez #manpasandshadi #horoscope #spiritual #lovelife #lovespell #marriagespell#aamilbabainpakistan #amilbabainkarachi #powerfullblackmagicspell #kalajadumantarspecialist #realamilbaba #AmilbabainPakistan #astrologerincanada #astrologerindubai #lovespellsmaster #kalajaduspecialist #lovespellsthatwork #aamilbabainlahore #blackmagicforlove #blackmagicformarriage #aamilbaba #kalajadu #kalailam #taweez #wazifaexpert #jadumantar #vashikaranspecialist #astrologer #palmistry #amliyaat #taweez #manpasandshadi #horoscope #spiritual #lovelife #lovespell #marriagespell#aamilbabainpakistan #amilbabainkarachi #powerfullblackmagicspell #kalajadumantarspecialist #realamilbaba #AmilbabainPakistan #astrologerincanada #astrologerindubai #lovespellsmaster #kalajaduspecialist #lovespellsthatwork #aamilbabainlahore #Amilbabainuk #amilbabainspain #amilbabaindubai #Amilbabainnorway #amilbabainkrachi #amilbabainlahore #amilbabaingujranwalan #amilbabainislamabad
Design and Analysis of Algorithms-DP,Backtracking,Graphs,B&B
Dynamic Programming
Backtracking
Techniques for Graphs
Branch and Bound
Democratizing Fuzzing at Scale by Abhishek Arya
Presented at NUS: Fuzzing and Software Security Summer School 2024
This keynote talks about the democratization of fuzzing at scale, highlighting the collaboration between open source communities, academia, and industry to advance the field of fuzzing. It delves into the history of fuzzing, the development of scalable fuzzing platforms, and the empowerment of community-driven research. The talk will further discuss recent advancements leveraging AI/ML and offer insights into the future evolution of the fuzzing landscape.
Water Industry Process Automation and Control Monthly - May 2024.pdf
Water Industry Process Automation and Control Monthly - May 2024.pdfWater Industry Process Automation & Control
Welcome to WIPAC Monthly the magazine brought to you by the LinkedIn Group Water Industry Process Automation & Control.
In this month's edition, along with this month's industry news to celebrate the 13 years since the group was created we have articles including
A case study of the used of Advanced Process Control at the Wastewater Treatment works at Lleida in Spain
A look back on an article on smart wastewater networks in order to see how the industry has measured up in the interim around the adoption of Digital Transformation in the Water Industry.Final project report on grocery store management system..pdf
In today’s fast-changing business environment, it’s extremely important to be able to respond to client needs in the most effective and timely manner. If your customers wish to see your business online and have instant access to your products or services.
Online Grocery Store is an e-commerce website, which retails various grocery products. This project allows viewing various products available enables registered users to purchase desired products instantly using Paytm, UPI payment processor (Instant Pay) and also can place order by using Cash on Delivery (Pay Later) option. This project provides an easy access to Administrators and Managers to view orders placed using Pay Later and Instant Pay options.
In order to develop an e-commerce website, a number of Technologies must be studied and understood. These include multi-tiered architecture, server and client-side scripting techniques, implementation technologies, programming language (such as PHP, HTML, CSS, JavaScript) and MySQL relational databases. This is a project with the objective to develop a basic website where a consumer is provided with a shopping cart website and also to know about the technologies used to develop such a website.
This document will discuss each of the underlying technologies to create and implement an e- commerce website.
The Benefits and Techniques of Trenchless Pipe Repair.pdf
Explore the innovative world of trenchless pipe repair with our comprehensive guide, "The Benefits and Techniques of Trenchless Pipe Repair." This document delves into the modern methods of repairing underground pipes without the need for extensive excavation, highlighting the numerous advantages and the latest techniques used in the industry.
Learn about the cost savings, reduced environmental impact, and minimal disruption associated with trenchless technology. Discover detailed explanations of popular techniques such as pipe bursting, cured-in-place pipe (CIPP) lining, and directional drilling. Understand how these methods can be applied to various types of infrastructure, from residential plumbing to large-scale municipal systems.
Ideal for homeowners, contractors, engineers, and anyone interested in modern plumbing solutions, this guide provides valuable insights into why trenchless pipe repair is becoming the preferred choice for pipe rehabilitation. Stay informed about the latest advancements and best practices in the field.
Gen AI Study Jams _ For the GDSC Leads in India.pdf
Gen AI Study Jams _ For the GDSC Leads in India.pdf
TECHNICAL TRAINING MANUAL GENERAL FAMILIARIZATION COURSE
AIRCRAFT GENERAL
The Single Aisle is the most advanced family aircraft in service today, with fly-by-wire flight controls.
The A318, A319, A320 and A321 are twin-engine subsonic medium range aircraft.
The family offers a choice of engines
Recently uploaded (20)
Quality defects in TMT Bars, Possible causes and Potential Solutions.
Quality defects in TMT Bars, Possible causes and Potential Solutions.
Halogenation process of chemical process industries
Halogenation process of chemical process industries
NO1 Uk best vashikaran specialist in delhi vashikaran baba near me online vas...
NO1 Uk best vashikaran specialist in delhi vashikaran baba near me online vas...
Design and Analysis of Algorithms-DP,Backtracking,Graphs,B&B
Design and Analysis of Algorithms-DP,Backtracking,Graphs,B&B
Water Industry Process Automation and Control Monthly - May 2024.pdf
Water Industry Process Automation and Control Monthly - May 2024.pdf
Final project report on grocery store management system..pdf
Final project report on grocery store management system..pdf
The Benefits and Techniques of Trenchless Pipe Repair.pdf
The Benefits and Techniques of Trenchless Pipe Repair.pdf
Gen AI Study Jams _ For the GDSC Leads in India.pdf
Gen AI Study Jams _ For the GDSC Leads in India.pdf
LIGA(E)11111111111111111111111111111111111111111.ppt
LIGA(E)11111111111111111111111111111111111111111.ppt
TECHNICAL TRAINING MANUAL GENERAL FAMILIARIZATION COURSE
TECHNICAL TRAINING MANUAL GENERAL FAMILIARIZATION COURSE
AUXILIARY CRANE INSPECTION CHECKLIST Form # HSEQ - AC Rev 2.docx
- 1. 1 AUXILLIARY CRANE INSPECTION CHECKLIST (To be completed on daily basis) Page 1 of 1 Form # HSEQ-AC (Rev 2 –Mar 23) Project Information Project Name: Tiara Hotel Auxiliary Crane No: 4/3.06/1 Location: Level 3 Date : 3rd Party Inspection of Auxiliary crane valid till: 26 August 2018 3rd Party certificate of operator valid till: Shift: (This checklist to be completed for both Shifts) Sr. Description S (Satisfactory) D (Deficiency) N/A Comments 1. Availability of Operators Manual and load chart 2. Maintenance Records 3. Operator Competency 4. Rigger Competency 5. Auxiliary Crane Section Condition 6. Structural Welds Physical Condition 7. Tie Bars and Pins 8. Foundation/Ballast 9. Earthing Condition 10. Hoist limits and breaks functioning 11. Slewing Gear 12. Drum and Wire Rope 13. Hook and Safety Latches 14. Main/luffing boom 15. Counter Jib 16. Counter weight secured 17. Pin and Bolts 18. Rope Sheaves 19. Safe Load Indicator 20. Radius Angle Indicator 21. Overload Cut-off device 22. Limit switches 23. Foundation bolts/ anchors 24. Effective means of communication 25. Fire extinguisher 26. Anti-collision system working 27. Valid Third Party Test and Inspection Certificates 28. Others ( Specify) Remarks: This checklist to be completed for both Shifts Operator Name: Signature: Reviewed By HSE Manager / In charge : Signature: Noted by Project Leader Signature: