Downloaded 1,089 times
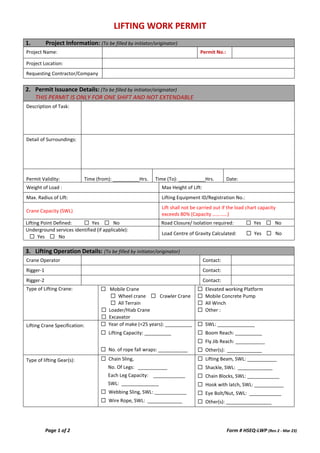
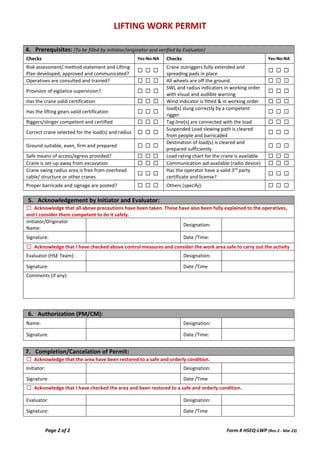

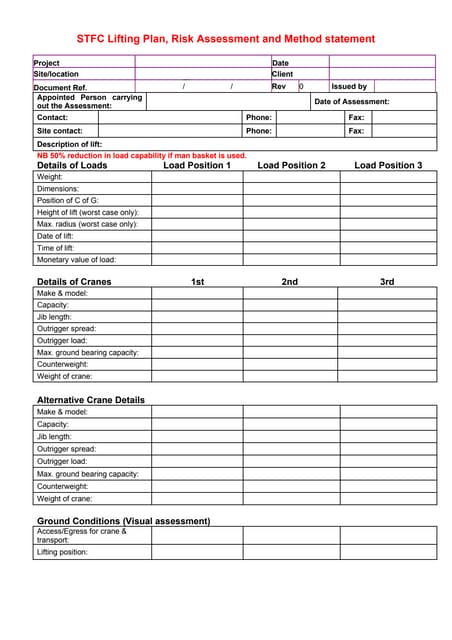
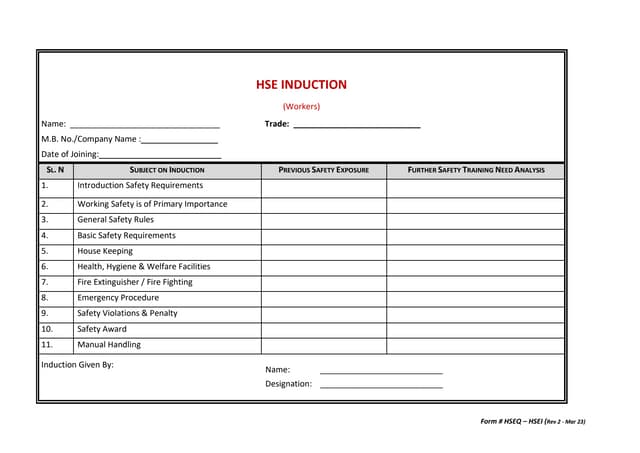
The document outlines a lifting work permit form that must be filled out by the initiator, detailing project information, permit issuance details, and lifting operation specifics. It emphasizes safety checks, risk assessments, and the necessary certification for cranes and lifting gear. Acknowledgment sections for initiators and evaluators ensure compliance with safety measures before the lifting operation commences.