Downloaded 278 times
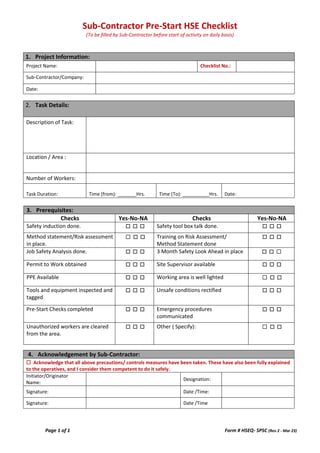

This document is a sub-contractor pre-start HSE checklist that must be filled out daily before starting any activity. It collects project information, task details including description, location, workers and duration. It also checks that various HSE prerequisites are in place such as safety inductions, risk assessments, PPE availability, inspection of tools and equipment, and that unsafe conditions have been rectified. The sub-contractor must acknowledge that all precautions and control measures have been taken and the workers have been deemed competent to perform the task safely.