Downloaded 81 times
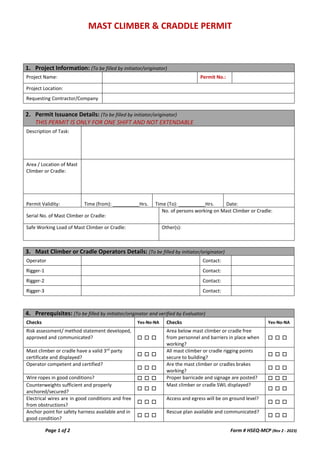
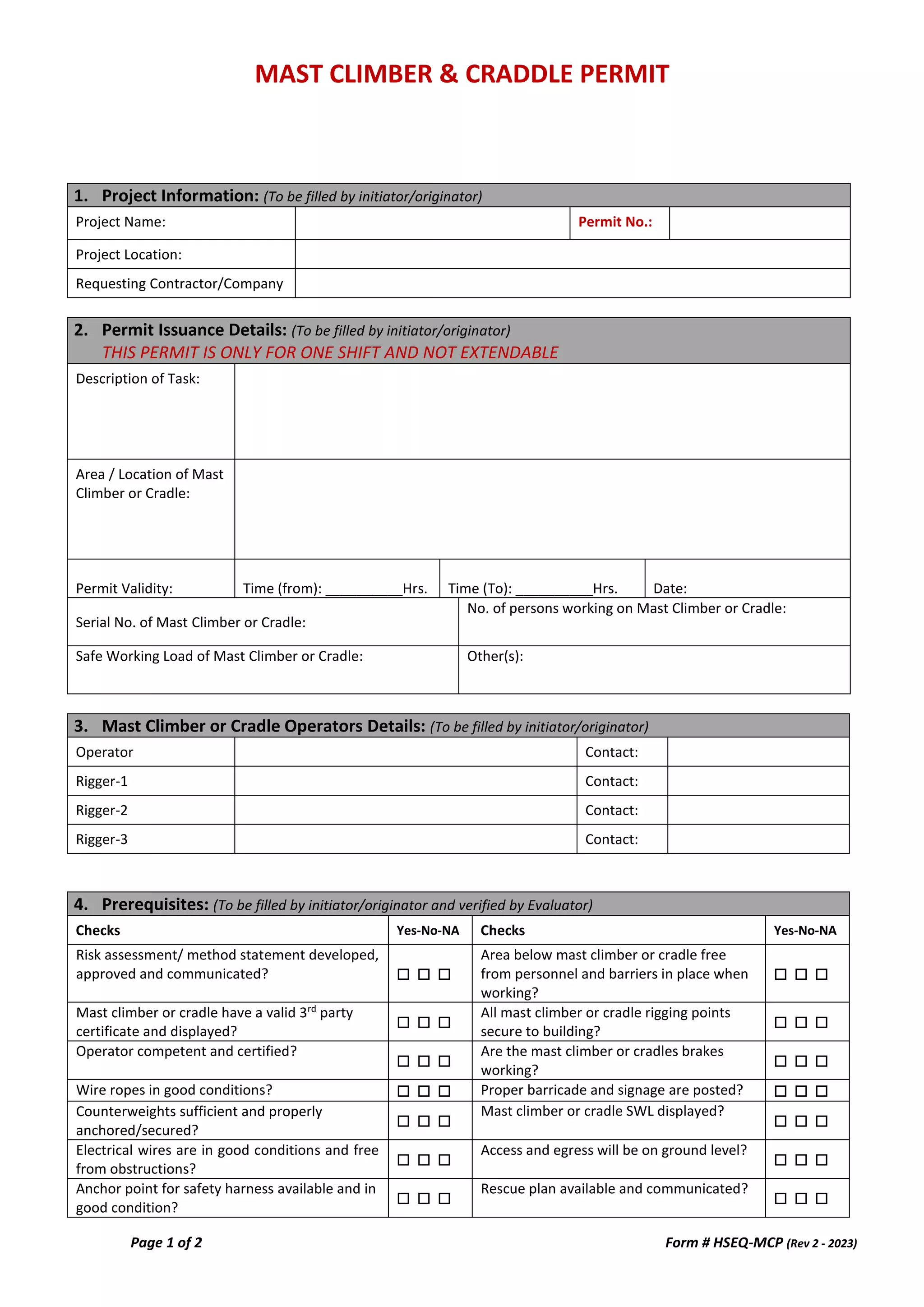
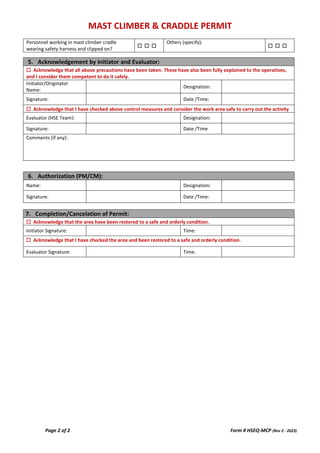

The document outlines a permit form for the use of a mast climber or cradle, including sections for project information, permit issuance details, operator information, and safety prerequisites. It emphasizes the importance of safety checks, operator competence, and equipment certification. Acknowledgement and authorization by the initiator and evaluator are required, along with a process for ensuring the work area is restored to a safe condition post-task.