Downloaded 165 times
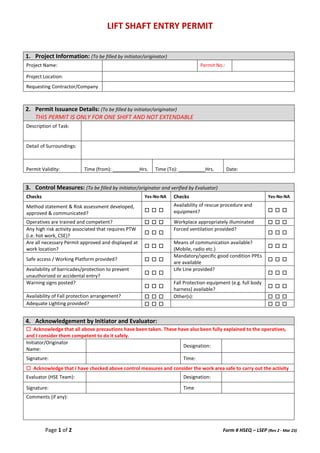
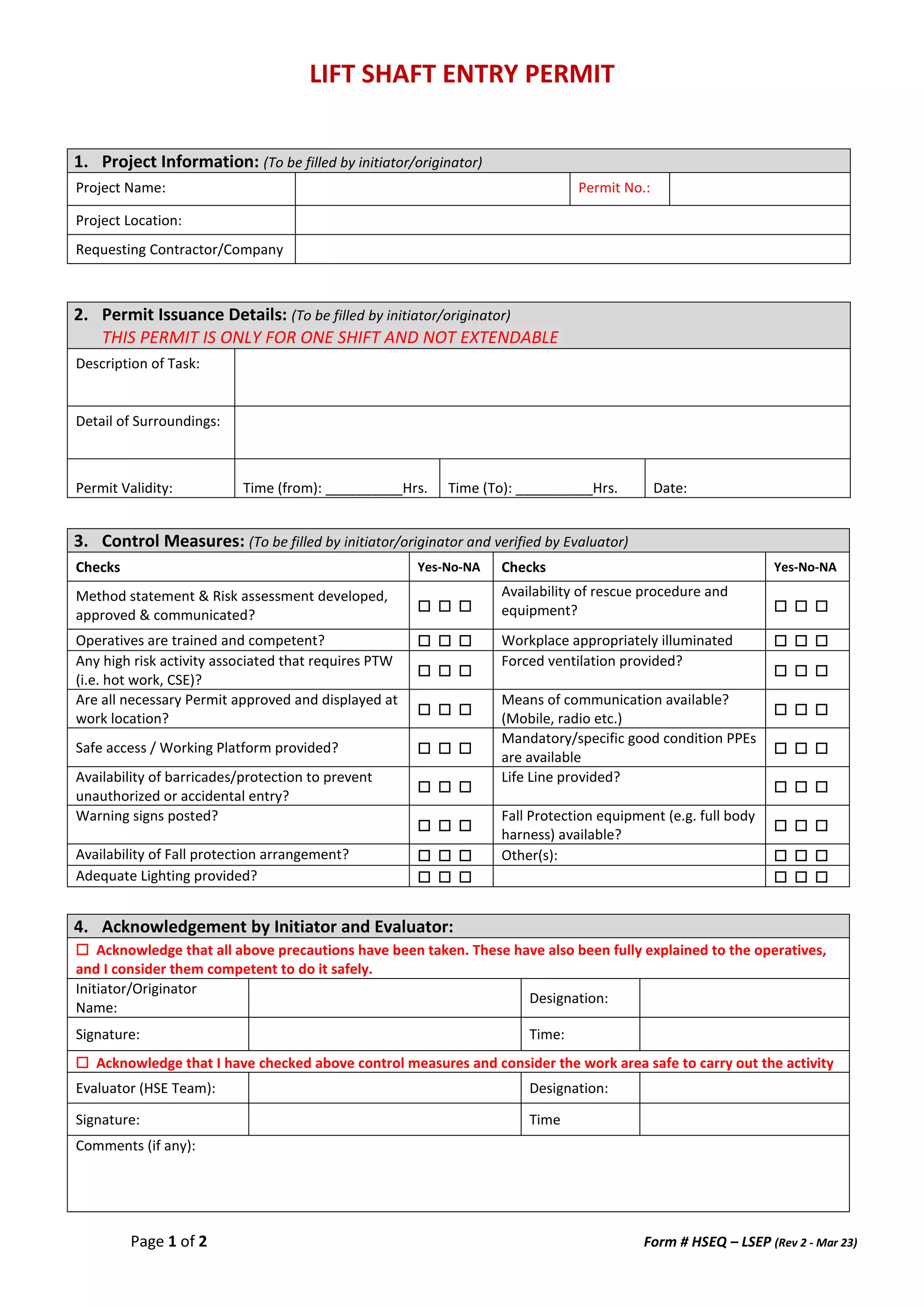

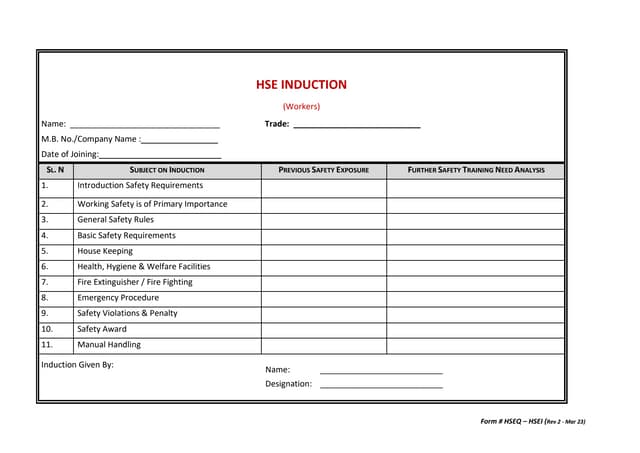
The document is a lift shaft entry permit form outlining project information, permit issuance details, control measures, and acknowledgments needed for safe operations. It requires confirmation of various safety checks and mandates permits for specific high-risk activities. The form also includes sections for authorization and completion verification.