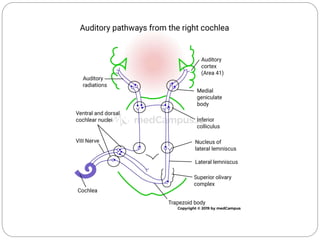
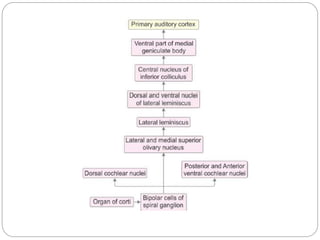
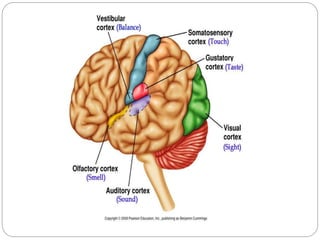
The auditory pathway consists of relay stations from the inner ear hair cells through the spiral ganglion, cochlear nuclei, superior olivary nucleus, lateral lemniscus, inferior colliculus, medial geniculate body, and auditory cortex. Sound is transmitted through these stations with the first order neurons in the spiral ganglion and higher order neurons at each subsequent station. There are three main types of hearing loss - conductive, sensorineural, and mixed. Conductive hearing loss interferes with sound conduction to the cochlea, sensorineural involves lesions of the cochlea/vestibulocochlear nerve, and mixed has both conductive and sensorineural components. Hearing is






















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)